Overactive bladder (OAB) affects 17-20 million Americans. It is characterized by the sudden urge to urinate with or without the loss of urine. This results in frequent urges to urinate usually both day and night. In many instances, there is an urge so strong that it results in loss of urine. The loss may be anywhere from a few drops of urine to the complete emptying of the bladder. This condition affects daily quality of life. People may avoid social interaction as well as curtail travel plans. Around 60% of OAB people are dry and have only urgency. The other 40% have urgency with incontinence.
Stress Urinary Incontinence (SUI) is a separate kind of urinary incontinence distinctly different from OAB. Stress incontinence is common in women after childbirth and in men after prostate surgery. Sudden cough, sneeze, or any sudden, unexpected movement leads to loss of urine. Usually, there is no associated urge to urinate.
Mixed incontinence is a combination of OAB and SUI. This occurs when a cough or sneeze pushes down on the bladder, and that pressure starts an uncontrollable bladder contraction or bladder spasm. To most patients, SUI and mixed incontinence appear to be the same.
The difference is significant in that OAB responds to medication, and SUI requires surgery to resuspend the bladder. To confuse things even more, bladder suspension surgeries that are tightened too much can convert SUI to OAB.
Overflow incontinence is associated with leakage from the bladder that is overfilled and incompletely emptied. Often, people have lost the sensation that they are full. They often leak at night, wetting the bed (enuresis). They may note leakage while sitting for long periods of time. They report getting up after sitting to find that the chair or sofa is wet, and they never felt the leakage.
Causes of OAB
The cause of OAB is not always obvious. The most common neurologic conditions that cause OAB are stroke, Parkinson’s disease, and a spinal cord injury. Multiple sclerosis and peripheral nerve damage in the lumbar spine can also cause OAB. Non neurologic causes are bladder cancer, prostate enlargement or BPH, and interstitial cystitis. Bladder stones and urinary infections may cause OAB symptoms. Some medications may induce OAB symptoms.
Symptoms of Overactive Bladder
Sudden urge to urinate
Urinating 2 or more times a night
Incontinence of urine
More frequent urination than 8 times per 24-hour period
Diagnosis of Overactive Bladder
The diagnoses of SUI and OAB are first separated by a complete history. A complete history will help answer the following questions:
When does it occur?
How long has it been going on?
Does it occur with change of position? Is it lying to sitting or sitting to standing?
Does it occur when you are running water in the sink or pumping gasoline into your car?
Does it wake you up at night needing to go to the toilet?
Does leakage occur without warning?
When going someplace new, is the location of the bathroom the first thing you look for?
Do you have blood in your urine?
Do you have painful intercourse?
Tests for Overactive Bladder
Urinalysis is used to look for blood and/or infection.
Noninvasive, painless bladder scanning is used to look for incomplete emptying. Catheterization is used in some offices if no bladder scanner is available.
Focused neurological examination may be needed.
Pelvic examination looks for leakage with cough and cystocele formation. Cystoceles form when the bladder falls into the vagina. This is most commonly found after childbirth.
X-rays may be ordered if the urinalysis is abnormal and the urine contains blood or shows signs of infection.
Cystoscopy may be needed to evaluate the inside of the bladder. This is an endoscopic inspection of the bladder lining. The evaluation looks for bladder stones, BPH, tumors, and signs of infection.
A urine cytology is used to check the urine for cancer cells.
Urodynamics or cystometrics can be used. This procedure fills the bladder with water and measures the bladder’s filling pressure and its response to filling, such as unstable bladder contractions.
Blood is drawn to assess kidney function and to look for diabetes.
Treatments for OAB
Medications
Medication is the first line of treatment for OAB and mixed incontinence. The bladder nerves are modulated by a chemical transmitter called acetylcholine. Acetylcholine attaches to the muscarinic (M2 and M3) receptors in the bladder to stimulate muscle contractions. The medications for OAB are called anticholinergic or antimuscarinic medications. These medications attach to the muscarinic receptors and block these bladder receptors thus blocking the bladder spasms. The commonly available medications are Detrol (Tolterodine), Ditropan and Gelnique (Oxybutynin), Enablex (Darifenacin), Levsin (Hyoscyamine), Sanctura (Trospium), Toviaz (Fesoterodine), and VESIcare (Solifenacin).
The major side effects of this group are constipation and dry mouth. Older drugs such as oral generic Oxybutynin have more of these side effects and have been associated with decline in cognitive function in the elderly. Dry mouth is common, and you should see your dentist every 6 months. Dry mouth leads to an increase in cavities and gum disease. Watch for signs of urinary retention or the inability to urinate. While retention is rare, it can occur. Men are more likely to have retention than women. In men, these medications are almost always used in combination with an alpha blocker such as Flomax (Tamsulosin) to prevent retention. Dry eyes may be noted and are treated with eye drops. Occasionally, the dry mouth causes you to drink more, and this increased fluid intake worsens OAB. Likewise, constipation caused by these medications can worsen OAB. Your insurance likely has a list of approved drugs. Not all people with OAB respond equally well to all medications. You need to ask your doctor for a trial of all medications available until you find one that works for you without excessive dry mouth or constipation. Once you find one with acceptable side effects, it will take several months for your system to fully calm down the OAB.
The newest addition to the OAB market is Myrbetriq (Mirabegron). This is a new class of drug called a beta agonist. It stimulates beta-3 adrenergic receptors. This relaxes the bladder avoiding the side effect of constipation that is so common among the anticholinergic drugs.
Behavioral Therapies for Overactive Bladder
Some people will benefit from changes in their daily routine. Avoidance of stimulants such as caffeine may reduce the number and intensity of the urges. Cutting back on alcohol intake also helps. Kegel’s exercises may be done for both SUI and OAB. Weight loss lessens the downward pressure the abdominal contents put on the pelvis and bladder. Keeping a voiding diary may give you insight into triggers for your OAB. Fluid management is helpful in some cases. Be sure not to cut back on fluids to the point of dehydration. Biofeedback helps some people learn to relax their pelvic muscles, and this lessens the urgency.
Avoiding spicy foods, acidic foods, alcohol, and caffeine-containing beverages may help.
Constipation should be prevented with an increased intake of fiber or with stool softeners. Constipation leads to an increase in frequency and urgency.
Neuromodulation of Overactive Bladder
Neuromodulation with implantable sacral nerve root stimulators may help people not responding to medications and behavioral modifications. The brand name for this device is an Interstim. This treatment relies on insertion of an electrode into the S3 sacral foramen to the 3rd sacral nerve root. This electrode is then hooked to a pacemaker-like generator. Before the permanent device is implanted, a temporary device is used for 4-5 days to see if the treatment is right for you. If you get relief, then the permanent generator is placed under the skin just like a pacemaker.
Botox Injection for Overactive Bladder
Recently, the FDA approved Botox for direct injection into the bladder. Its role in OAB is not yet fully worked out. The dosing schedule is about every 4-6 months. It requires the direct injection of Botox into about 20 sites in the bladder wall. In some studies, it was shown as many as 30% of patients develop urinary retention. They must then learn to do self, clean, intermittent catheterization on themselves.
Surgery for Overactive Bladder
In women having prolapse of the bladder, surgical repair to support the bladder may relieve urgency. Mild cystoceles that undergo repair may or may not relieve urgency with incontinence. Occasionally after SUI surgery, OAB symptoms will start or worsen especially if the sling is too tight or if there is postoperative urinary retention.
Kidney cancer affects about 20,000 men and 12,000 women per year. Kidney cancer is called Renal Cell Carcinoma(RCC). It is a type of cancer called adenocarcinoma. This is a distinctly different cancer than that originating from the lining of the kidney’s collecting system. The cancer of the lining of the collecting system is a Transitional Cell Carcinoma(TCC). Transitional Cell Carcinoma is similar to bladder cancer and is discussed under that section of the web site.
The kidneys are 2 paired organs in the area on the back above the waist protected by the two lower ribs. The kidney’s purpose is to filter the blood and remove metabolic waste products from the blood. Once urine if formed, it travels down the ureter to the bladder. Urine is then stored in the bladder until there is an appropriate time to empty the bladder.
Risk Factors
Certain life styles, occupational exposure, and diseases may increase the chance that you may develop renal cancer. Of course, all people falling within a risk category will not develop cancer. These factors just predict a higher chance of developing cancer in those people than in people without these risk factors. People without risk factors can still develop kidney cancer.
Smoking not only increases the risk of kidney cancer or adenocarcinoma but also of developing transitional cell carcinoma.
Obesity, high caloric intake, and a diet high in fried meats are risk factors.
Over the counter medications such as NSAIDS (Ibuprofen, Naproxen) has been found to increase one’s risk. Phenacetin, which is no longer on the market, was a risk previously.
Asbestos and cadmium exposure in the work place, as well as Coke, used in the iron and steel industry may increase your risk.
People with high blood pressure are at increased risk.
Those with a family history of kidney cancer have an increased risk.
People with chronic kidney disease, as in dialysis patients, have an increased risk.
Von Hippel-Lindau disease and tuberous sclerosis are inherited disorders that show an increased risk for developing cancer.
Men are at greater risk than women.
Symptoms
Blood in the urine
Abdominal pain high in the abdomen
Abdominal mass high in the abdomen
Unexplained, intermittent fevers
Unexplained loss of appetite
Unexplained anemia
Weight loss without dieting
New onset of high blood pressure
Lab Findings
High serum calcium
Anemia
Increased liver function tests
Increased sedimentation rate
Increased alkaline phosphatase
Elevated white blood count without infection
Diagnosis and Testing
Many kidney cancers are now found as an asymptomatic mass on CT scans done for other causes. This finding is then confirmed by additional X-rays or blood tests. Most renal cell carcinomas are distinctive enough on CT scans done without IV contrast then repeated with IV contrast that they do not require biopsy. These masses enhance with contrast injected into a peripheral vein. This enhancement confirms this is a mass and not a cyst.
In people with poor kidney function that cannot have a CT with contrast, a renal ultrasound may confirm this is a solid mass. Occasionally, an MRI is required to help with the diagnosis.
IVP or intravenous pyelogram and arteriography are rarely used today in diagnosing renal masses.
Blood chemistry and CBC are obtained to evaluate for abnormal levels of liver enzymes, increased calcium in the blood, increased alkaline phosphatase from bone, and a CBC to look for anemia.
Physical exam usually fails to find any abnormality in the early stages of renal cancers. These masses can become quit large and still remain confined to the kidney without spreading or metastasizing.
A biopsy is occasionally used when the X-ray diagnosis is not completely clear, but a biopsy is not routinely done. These tumors are very vascular, and the larger ones have bleeding after a biopsy that rarely leads to an emergency kidney removal. Findings show that 80-85% of renal masses are cancers, and they must be removed. Oncocytomas are benign solid tumors of the kidney but cannot reliably be differentiated from cancers by needle biopsy. There are rare reports of needle biopsy causing local spread of an otherwise contained cancer. Smaller, indeterminate masses do not have as much of a tendency to bleed following biopsy.
Staging of Renal Cell Carcinoma
TNM staging
T1
T1a : limited to kidney < 4 cm
T1b : limited to kidney > 4 cm, < 7 cm
T2 : limited to kidney > 7 cm
T3 : tumour / tumour thrombus extension into adrenal or renal vein or perinephric tissues (but contained by Gerota’s fascia)
T3a : spread to perinephric fat
T3b : spread to renal vein or intra diaphragmatic IVC
T3c : spread to supra diaphragmatic IVC
T4 : beyond Gerota’s fascia.
N0 : no nodal involvement
N1 : single regional lymph node involved
N2 : beyond N1 (NB laterality does NOT affect nodal staging)
M0 : no distant metastases
M1 : distant metastases
Stage groupings
stage I : T1 N0 M0
stage II : T2 N0 M0
stage III : Everything between II and IV
stage IV : any one of : M1 or N2 or T4
Stage groupings
stage I : T1 N0 M0
stage II : T2 N0 M0
stage III : Everything between II and IV
stage IV : any one of : M1 or N2 or T4
Grade of Renal Cell Carcinoma
Clear Cell RCC –This cell type makes up about 80 % of all renal cell carcinomas. On microscopic evaluation, these tumor cells appear very pale or clear.
Papillary RCC –This cell type makes up 10-15 % of kidney cancers. These cancer cells usually develop finger-like projections in the tumor.
Chromophobe RCC –These cells appear to be larger than those of clear cell carcinoma but are still clear.
Collecting Duct –These cancers are only about 1% of renal cell cancers but are considered aggressive tumors. This cancer forms irregular tubes inside the tumor.
Unclassified RCC –While rare, these do not fit any of the above subtypes or are composed of multiple subtypes.
Treatment of Renal Cell Carcinoma
Open Nephrectomy for Renal Cell Carcinoma
The primary treatment of renal cell carcinoma has always been surgical removal of the kidney. This is called radical nephrectomy. This involves the removal of the entire kidney including Gerota’s fascia, the fatty tissue around the kidney. The lymph nodes in the central portion of the kidney are removed also. Sometimes the lymph nodes between the aorta and vena cava are sampled as well. The adrenal gland on the same side as the tumor has also traditionally been removed. The adrenal gland is no longer routinely removed.
The need for whole kidney removal was driven by the late stage in which most patients presented to the doctor. With CT scanners now in every hospital and emergency room, these tumors are often now found at an earlier stage while looking for other intra-abdominal problems.
Now that these tumors are smaller, there has been a shift to partial nephrectomy where just a portion of the kidney is removed. If the tumor is small, < 5cm, and is on the upper or lower portion of the kidney, only that portion of the kidney containing the tumor may be removed. Current technology does not allow for the removal of centrally located tumors.
Partial Nephrectomy for Renal Cell Carcinoma
The open surgical approach was through the bed of the removed 11th rib. This incision was about 10 inches long and recovery was moderately painful. With the introduction of laparoscopy, the kidney is now removed through a small incision in the front of the abdomen. You just need an incision large enough to get the kidney out, usually the incision is about 4 inches in length.
Now it is also possible to do this laparoscopic approach for partial nephrectomy. Robotic surgery is a refinement of the laparoscopic approach. The surgical robot is occasionally used to do nephrectomies and partial nephrectomies. It does not offer as much advantage to these operations as it does for prostatectomy.
Cryotherapy for Renal Cell Carcinoma
Cryotherapy is the freezing of these cancers using insertion of cryo-needles that are cooled with liquid helium. There is a freeze, thaw, refreeze, thaw cycle. The freezing alone may cryo preserve some of the cells. Thawing rapidly causes the ice crystals in the cells to rupture and kill the cells. Tumors larger than 5 cm are not amenable to cryotherapy.
Radiofrequency Lesioning (RF) for Renal Cell Carcinoma
Radiofrequency lesioning uses the same size criteria as cryotherapy. Instead of freezing the tumor, it is heated, and essentially the tumor is cooked, killing that portion of the kidney containing the tumor.
Embolization for Renal Cell Carcinoma
Embolization may be used for patients too ill for other surgeries. Much like a heart catheterization, a catheter is introduced through the groin into the renal arterial branch feeding the tumor, and the blood flow is blocked. This causes the tumor to die. There may be incomplete destruction of the tumor, and occasionally, there may be damage to the adjacent, normal kidney.
Radiation Therapy for Renal Cell Carcinoma A
Radiation therapy has little effect on renal cell carcinoma in the kidney. It is primarily used to treat the spread in the bones and other organs experiencing pain.
Chemotherapy for Renal Cell Carcinoma
Chemotherapy has never had much effect on renal cell and is not routinely used.
Immunotherapy for Renal Cell Carcinoma
Immunotherapy dates back to the 1980s. This was the first treatment to show an increased survival rate. Immunotherapy is sometimes used to slow the growth of the tumor. Interferon was the first attempt at slowing the growth after the tumor had spread. The major side effects were the feeling of flu-like symptoms. Interleukin-2 (IL-2) has also been used both alone and in combination with Interferon.
More recently, targeted therapy with Sutent (sunitinib), Nexavar (sorafenib), Votrient (pazopanib), Afinitor (everolimus), and Torisel (temsirolimus) have most recently been utilized to slow the in-growth of blood vessels into the tumor starving it of its blood supply.
Life with One Kidney
One kidney is enough for most people to live a normal life. Partial nephrectomy removes less of the total renal function than nephrectomy does. Partial nephrectomy may only remove the diseased, nonfunctioning portion and have little reduction in total renal function.
Monitoring of Renal Cell Carcinoma
Follow-up blood work and CT scans with chest X-rays to monitor for spread of the cancer after removal are routinely done for 3-5 years depending on the pathologic stage and the results of the CT scans themselves.
Interstitial Cystitis (IC) is also referred to as Painful Bladder Syndrome (PBS) or Chronic Pelvic Pain. All three of these things refer to the same thing, so for simplicity we will refer to it simply as IC, the acronym for Interstitial Cystitis. IC is a disease that mostly affects women, but some men also have this condition.
IC is usually initially treated as a form of recurrent UTIs in women or prostatitis in men. There appears to be about a 4:1 ratio of women to men. When the recurrent “UTI” fails to respond to treatment, the patients usually end up at the urologist for men and the gynecologist for women. Women, after being determined by their gynecologist to not have endometriosis, pudendal nerve neuralgia, endometriosis, pelvic floor dysfunction, or pelvic congestion syndrome, are subsequently referred to the urologist.
Acute Cyastitis
Interstitial cystitis is a poorly understood chronic pain in the pelvis or vagina. It frequently runs in families and may be genetic. As the cause is unknown, there have been studies that link IC to pelvic trauma, chronic overdistension of the bladder, repeated UTIs, genetic factors, and autoimmune factors. It may be a genetic deficiency of the glycosaminoglycan layer of protection on the bladder surface. Symptoms may be mild for many years before becoming painful. Often these women just seem to urinate frequently. Some women urinate as often as every hour by day and every several hours at night in the most severe cases. Like small children, I find some mothers who knew every available restroom in town. As the disease progresses, the pelvic pain increases as does the frequency and urgency to urinate. It is often associated with dyspareunia or painful intercourse. The pain after intercourse may last for days. Initially, antibiotics make them feel better. Soon they note that as soon as the antibiotics stop the pain is back in just a day or two. Their urine cultures are usually negative. Often, their doctor has called them back and told them nothing grew on the culture but to continue the antibiotics. Many of these women want to be on continuous antibiotics, but this is not an appropriate treatment.
In men, IC acts as a mimic for prostatitis and is associated with painful ejaculation and occasionally as an isolated, unilateral, or bilateral testicular pain. The same is true in its response to antibiotics as it is with women. There is some relief of the symptoms while taking antibiotics. Usually, the pain has been progressively increasing for months or years. Men come in when there has been a recent, sudden increase in frequency or intensity of the symptoms.
Evaluation of Intersitial Cystitis (Or Painful Bladder Syndrome)
The best place to start is to discuss this with a physician that treats IC. Much of the diagnosis is ascertained by a thorough history. The urologist will ask about frequency of urination, urgency by day, and nighttime urination or nocturia. They will try to find out if there is a history of culture documented UTIs. A sexual history of increasing painful intercourse is important.
Associated illnesses include migraine headaches, irritable bowel or IBS, and autoimmune diseases. It is not currently known how they are related to IC, but some studies have found that 33% of IC patients also have IBS and migraines. Fibromyalgia may be increased in IC patients. This is a condition of increased pain over muscles and soft tissue that leads to sleep disturbance and fatigue.
For some time, insurance denied the existence of IC and required that a bladder biopsy with hydrodistention take place before they would approve the medications to treat IC. Hydrodistention is the stretching of the bladder under anesthesia to measure the capacity of fluid that the bladder would hold. This was felt to be both diagnostic and therapeutic. The IC bladder usually has a diminished capacity to stretch even under general anesthesia. The lining or mucosa frequently becomes reddened and there may be submucosal hemorrhages called glomerulations.
Identification of a Hunner’s ulcer is diagnostic of IC if no other pathology is present. Occasionally, gross bleeding occurs during hydrodistention. If biopsies are taken, they usually show increased chronic inflammatory response in the submucosal areas of the biopsy. Giemsa stains show increased numbers of mast cells in the sub mucosa. These cells contain many histamine granules. This histamine is the same as that which causes nasal congestion with allergies. Biopsies may show erosion of the mucosa as well.
Other Diagnostic Tests for IC or PBS
Potassium sensitivity testing has been around for many years. It was one of the earlier tests for IC. The test is preformed by inserting a small catheter into the bladder. First, a saline solution is instilled under gravity to measure your pain response. This is then drained from the bladder, and a potassium-based solution is instilled. A positive test consists of increased pain with the potassium solution. I have never been a fan of this test.
Installation of a rescue treatment is the alternative option. A solution of medications is instilled into the bladder to see if this combination of bicarbonate, Lidocaine, and heparin temporarily relieves the pain. The bicarbonate of soda solution neutralizes the acid in the urine. The Lidocaine numbs the bladder and works best when the acid in the urine has been neutralized. The heparin is an anticoagulant injection that in this case is used to coat the inside of the bladder. Heparin is felt to replace the missing glycosaminoglycan layer on the bladder surface. In mild to moderate cases of IC, the patients will see relief of their pain in 15-20 minutes, and it may last for many hours. In severe cases of IC, there may be relief, a little relief, no relief, or rarely temporary worsening of the pelvic pain.
Treatment for Chronic Pelvic Pain
Treatment after diagnosis begins with dietary and behavioral modifications.
Many foods may make IC symptoms worse. As a general rule, if it burns your mouth, it may cause bladder irritation. Spicy foods such as peppers and spices may flare-up your IC.
Acidic foods such as carbonated drinks, orange juice, lemonade, grapefruit juice, tomato juice, tomatoes, or tomato sauce may also cause IC symptoms flare-up. Caffeine containing foods such as coffee, tea, sodas, and chocolate may act as stimulants that may cause bladder irritability. While not a food group, over the counter decongestants can cause worsening of IC. These medicines act as stimulants just like caffeine.
Foods high in potassium like bananas and Lite Salt often worsen IC symptoms.
Learning to deal with stress can lessen IC symptoms in both frequency and severity. Stress is often associated with bad situations, but “happy” stress affects IC as well. Both types of stress include adrenaline release. The stimulant affect of this causes an increase in the frequency of urination and the pain of IC. As above in the caffeine section, decongestants fit into this category.
Pelvic relaxation techniques and meditation may help with IC symptoms.
Medications for IC or Chronic Pelvic Pain
When dietary and behavioral modification does not help enough, medications may be prescribed.
The earliest treatments for a painful bladder are no longer used. These included the introduction of a silver nitrate solution into the bladder. This was used to strip off the lining of the bladder. It was thought that when the lining regrew it would be normal. Clorpactin or oxychlorosene was also used for the same purpose, though these treatments have not been used in 10-20 years.
Rimso-50 was the first FDA approved treatment for IC. DMSO or dimethyl sulfoxide (Rimso-50) was used as a topical treatment instilled into the bladder as an anti-inflammatory or antihistamine treatment. It was used alone or in combination with heparin. This is rarely used anymore. The main complaint from people using it was the strong odor of garlic their body emitted for 24-48 hours after each treatment. Liver function testing should be done on patients requiring weekly use of DMSO.
Elmiron (Pentosan Polysulfate Sodium) is an oral medicine found to be excreted in the urine that coats the bladder as a replacement for the missing or thin layer of glycosaminoglycans. Recoating the bladder is similar to a mother’s use of Desitin Ointment in the treatment of a baby’s diaper rash. The layer of Elmiron keeps the urine from touching the bladder and causing inflammation. For people that cannot take this orally, it is sometimes used as part of the IC rescue cocktail in place of heparin. Occasionally, some women experience side effects of nausea or reversible hair loss. Elmiron may take up to 6 months to work, and most people are impatient and come off of the Elmiron before it has a chance to work. The other drawback is the cost of over $400 per month.
Elavil (Amitriptyline) is a tricyclic antidepressant that suppresses pain by way of the serotonin pathway. It also exerts a direct relaxing effect upon the bladder. It relaxes the bladder by affecting the anticholinergic nerve pathways much as the newer overactive bladder medications work. Many IC patients exhibit fatigue due to nighttime urination and lack of sleep. Amitriptyline has a sedating effect and helps restore sleep. Related drugs such as Pamelor or Nortriptyline may be better tolerated if the Amitriptyline is too sedating.
Atarax (Hydroxyzine) is a very old, first generation, antihistamine that is used both for its antihistamine and sedating properties. Remember, mast cells in the bladder lining are full of histamine and are associated with IC on bladder biopsy. While the second generation Benadryl, third generation Zyrtec, and Claritin are also antihistamines, they are much less potent. They may or may not work as well as Atarax.
Overactive bladder medicines may be used but are less effective in treating IC than in true overactive or spastic neurogenic bladders. This class of medications includes VESIcare (Solifenacin), Enablex (Darifenacin), Toviaz (Fesoterodine), Sanctura (Trospium), Detrol (Tolterodine), and Ditropan (Oxybutynin). All are antimuscarinic or anticholinergic medications.
Pyridium (Phenazopyridine) also found in AZO over the counter may help with IC pain. It is an azo dye that acts as a topical anesthetic in the bladder when taken orally.
Many names have come and gone for the medical combination of methylene blue for anesthesia, Hyoscyamine an anti spasmodic, a salicylate for pain, and methenamine as a urinary antiseptic. Urised, Prosed, Prosed DS, Uribel, Utira C, are all essentially the same medication.
Alternative medications used include: aloe vera cactus capsules, chondroitin, and Prelief. I am sure there are others. There is little data to support their benefits, but I do have patients who swear by them.
Postmenopausal women present similarly but frequently get better on vaginal estrogen cream as a topical therapy. While IC or interstitial cystitis may take months to control, estrogen deficiency is usually better in 2-3 weeks or less with estrogen replacement therapy.
Bladder cancer typically refers only to Transitional Cell Carcinoma (or TCC) of the bladder. This type of cancer makes up 90-95% of all bladder cancers. Squamous cell carcinoma makes up only about 5% of bladder cancers. Adenocarcinoma occurs only about 2% of the time.
Since transitional cell is the most common cell type and presents about 70,000 new cases a year with 14,000 deaths in 2010, this article will only deal with Transitional Cell Carcinoma.
The empty bladder is a hollow, potential space organ similar to an empty balloon in the pelvis. Its function is to store urine between urinations. The bladder, as well as the ureters, is lined with a tissue type called transitional cells. This name comes from the fact that the bladder lining or urothelium is 7 layers of cells thick. The bottom layers are rounder and transition (or change) into flatter cells at the surface of the bladder.
The lamina propria is the layer just beneath the bladder mucosa or urothelium. (When you pull the skin off the chicken, the thin white layer that you see underneath the chicken’s skin is pretty much what we’re talking about.) This thin layer attaches the urothelial layer to the deeper underlying muscle layer. The muscle layer is the layer that contracts to allow the urine to flow out from the bladder at the time of urination.
Example of Bladder Tumor (Cancer) in Female
Example of Bladder Cancer (Tumor) in Male
Signs and Symptoms of TCC
The most common sign of bladder cancer is hematuria. Hematuria is the presence of blood in the urine. This may be visible to the naked eye as gross hematuria or microscopic and can be detected by your doctor upon urinalysis. Hematuria itself does not mean that you have cancer but does warrant an evaluation. While infection, stones, and prostate enlargement are more common than cancer, it is most important to find a cancer early.
Frequent urination may be a sign of bladder cancer. When this is new in onset and coupled with blood in the urine, tests for cancer are ordered.
Painful urination or pain in the pelvic area may also occur.
Dysuria or burning on urination may occur without infection or kidney stones.
Causes of Bladder Cancer
The kidneys eliminate waste products. These waste products are held in the bladder between urinations. The longer the urine is held the longer it is kept in contact with the urothelium.
Tobacco exposure is the most common cause of bladder cancer accounting for over 50% of all cases in the USA. The most literature available on this particular cancer deals with smoking. There is literature to support that tobacco in any form can initiate the formation of bladder cancer. Chewing tobacco and snuff are not safe alternatives to smoking. The ratio of men to women with TCC is about 3:1. Many people feel that secondhand smoke is also a cause for TCC.
Chemical exposure in industry is the next most common cause. Most of this is due to hydrocarbon exposure. Most commonly, this occurs in any form of mechanical work.
Solvents made from oil are another source of exposure. Benzene and Naphthalene are known bladder carcinogens.
The tire and rubber industry utilizes oil in their manufacturing process. Even the handling of the finished product without gloves over long periods of time may cause cancer.
People in industries using dyes have an increased risk of developing bladder cancer. The worst dyes are called aniline dyes. Dyes used in the leather industry, textile industry, paint industry, and hair dye industries have been implicated.
Prior radiation exposure to the pelvis in the treatment of prostate, colon, and GYN cancers has been reported to increase the later risk of developing bladder cancer.
Chemotherapy exposure to cyclophosphamide has been shown to increase the risk of bladder cancer.
Age over 80 years is apparently an independent risk factor, even in the absence of any chemical or tobacco exposure.
Bladder stones, chronic urinary catheters, and a Middle Eastern parasite, schistosomiasis, are all risks for squamous cell bladder carcinoma.
Prevention of Bladder Cancer
You may have heard that you should drink 2 liters of water a day, but water contained in the foods you eat counts as part of that fluid intake. So, the most correct way is to tell you to eat and drink enough fluid to produce two liters of urine a day. Doing this keeps the urine diluted and decreases the time that any of the known carcinogens are in contact with the bladder lining.
Wearing appropriate barriers, when handling these chemicals, significantly reduces the risk of developing cancer. Gloves, respirators, and protective clothing requirements when handling chemicals are available in every work place in the MSDS (Material Safety Data Sheet) file required by OSHA (Occupational Safety and Health Administration).
Stopping all use of tobacco for 5-10 years reduces the risk of smokers to that of a non-smoker.
Thus far, large studies have not found any conclusive evidence that any dietary supplement decreases your risk of bladder cancer.
Healthy eating habits with foods low in fat and red meat but high in fruits and vegetables as well as weight loss have been shown to lower the risk of all cancers.
Diagnostic Evaluation
Once hematuria (or blood in the urine) is documented, a thorough history looks at occupational and tobacco exposure risk factors.
X-rays look for abnormalities of the lining of the kidneys, ureters, and bladder. The older x-ray was the intravenous pyelogram. The newer x-ray is the CT (computed tomography) urogram. Both require the injection of an iodine containing contrast. The contrast is excreted in the urine and outlines the internal collecting system of the kidney, ureters, and bladder. The CT can also evaluate the bladder wall thickness and look for any signs of a tumor spreading to the pelvic lymph nodes. IVP only looks at the collecting system and not the lymph nodes or adjacent pelvic structures.
Cystoscopy is the telescopic visual inspection of the inside of the bladder. This finds tumors that are too small to see on an x-ray evaluation. So far, we have not been able to find a substitute for this direct visual inspection of the bladder.
Ureteroscopy is the visual evaluation of the inside of the ureters for a tumor. This is done when the x-rays suggest abnormalities in the ureters and/or kidneys. About 3% of TCC is found in the upper urinary tract above the bladder.
Urinary cytology is the microscopic inspection of the urinary sediment. The urine is concentrated in a centrifuge, and the last drop is stained with the Pap (Papanicolaou) stain. This is the same process as for cervical Pap smear stains in women. The pathologist then evaluates the slide visually looking for cancer cells. Slow growing TCC sheds normal looking cells and may be missed. Sometimes the pathologist simply notes too many cells to be normal. The cytology is better at looking for the high-grade or more malignant cancers.
Tumor markers such as NMP-22, BTA STAT, and FISH assay may sometimes be helpful. They have not yet to date found a reliable enough tumor marker to replace the cystoscopy.
Rectal exam in men and pelvic exam in women evaluate for thickening of the pelvic tissues or fixation to the surrounding tissues that might suggest a more advanced tumor stage.
Staging
Initial staging or clinical staging of bladder cancer is done through physical findings and x-ray findings. The pathologist then evaluates the type of cancer and depth of bladder wall invasion using the TNM (tumor nodes metastasis) staging system to find the pathologic stage.
Staging of primary bladder cancer tumors (T)
Ta: Noninvasive papillary carcinoma
Tis: CIS (anaplastic “flat tumor” confined to urothelium)
Grade 1, or a low-grade tumor, has fairly normal looking cells still trying to form normal layers. These often form finger-like projections on stalks similar but finer than on a head of a broccoli floret. Frequently these tumors have a small stalk-like attachment to the bladder with a larger head of tumor on the end of that stalk. These often have 6-7 layers like normal transitional cell layers.
Grade 2, or moderately differentiated tumor cells, is more abnormal than grade 1. This often forms stubbier fingers with fewer layers. They in general have a broader base attachment to the bladder than does the grade 1 tumor.
Grade 3 tumors are classified as aggressive or poorly differentiated tumors. These are also referred to as high-grade tumors. They have very abnormal looking cells under the microscope. These are more likely to be multi-focal and low growing with a large, wide base. They generally are flatter tumors seen on cystoscopy.
Treatment of Bladder Cancer
The initial treatment is the TURBT or transurethral resection of the bladder tumor. This provides tissue for the pathologist to evaluate for tissue cell type, grade of the tumor, and depth of invasion or pathologic stage of the tumor. Bladder biopsies of the right, left, posterior bladder, bladder dome and trigone, and possibly the prostatic urethra in men are obtained to evaluate the remainder of the “normal” looking bladder for signs of pre-cancerous changes.
Mitomycin C may be placed in the bladder at the time of tumor resection in an attempt to reduce tumor recurrence.
Stage 1 tumors or T0, Ta, and Tis are localized to the top layer of the bladder lining and are removed by surgery and may require nothing more than close follow-up. They usually do not require any topical or intravesical chemotherapy.
Stage 2 or T1 tumors begin to invade the lamina propria or connective tissue layer below the urothelium but are not deep enough to penetrate into the bladder muscle. These have a higher recurrence rate and progression to higher-grade tumors and are usually treated with liquid chemotherapy introduced into the bladder by way of a catheter.
Stage 3 or T2 tumors invade into the muscle and are at risk for local or even wide spread systemic metastasis. This is currently treated with pre-op chemotherapy and bladder removal or cystectomy.
Stage 4 tumors have invaded through the bladder and into the fat surrounding the bladder or have spread to the pelvic lymph nodes or beyond. This is usually treated with IV chemotherapy and radiation.
Cystectomy and Urinary Diversion for Bladder Cancer
Once the bladder is removed, the urine must still be collected and disposed of. There are 3 main operations for this.
Ureterosigmoidostomy was the first attempt to divert the urine. The ureters were simply sewn into the distal colon. Most people had 3-6 loose bowel movements per day, but were continent of urine. This was discontinued when it was found that after 10 years or so these people developed colon cancer due to the interaction of the urine and the bacteria housed in the normal bowel movement.
Ileal conduit construction goes back to the 1950’s. This is constructed by disconnecting a segment from the bowel as an isolated segment. This utilizes a 6-8 inch segment of small bowel to bring the urine to the skin. The urine is then collected in an ostomy bag.
Neo bladder is the construction of a new bladder-like pouch that is connected to the urethra and allows for some semblance of normal voiding.
Orthotopic neobladders are new bladder pouches not sewn to the urethra but brought out of the skin through a catheterizable stoma.
Intravesical Therapy for Bladder Cancer
The introduction of chemotherapy or immunotherapy into the bladder in an attempt to decrease the rate of recurrence and progression to a higher stage of tumor is considered intravesical therapy.
Thiotepa was used until the 1980’s. It was replaced by chemotherapy after it was found to suppress bone marrow production in 13% of those patients.
Mitomycin, Adriamycin, and Doxorubicin are true chemo therapeutic agents used in the bladder.
BCG (Bacillus Calmette-Guerin) is a form of immunotherapy introduced in the 1980’s. It uses the introduction of a weakened strain of bovine tuberculosis to stimulate your own immune system to fight the cancer and reduce the chances of recurrence of a tumor. The side effects are flu-like symptoms, burning on urination, and frequent urination. It significantly reduces the rate of recurrence.
Intravenous Chemotherapy for Bladder Tumors
Until the introduction of IV chemotherapy, once the tumor had spread, the average life expectancy was about 18 months. With the introduction of MVAC, this began to climb.
M= Methotrexate
V=Vinblastine
A= Adriamycin or Doxorubicin
C= Cisplatin
Most recently, Gemzar or Gemcitabine and Cisplatin have replaced MVAC. This combination has a lower side effect profile than MVAC.
Carboplatin may be used if the renal function is decreased and Cisplatin cannot be used.
Long-Term Follow-Up After Bladder Cancer
Most patients need 5-10 years of long-term follow-up. This includes cystoscopy every 3 months for 1-2 years, then every 6 months for 1 year, and then yearly for 10 years for tumors localized to the bladder and treated with BCG.
Cystectomy patients with neobladders and orthotopic pouches need scope evaluations yearly.
Cystectomy and IV chemotherapy patients may be followed with CT scans, MRI (magnetic resonance imaging), and bone scans.
Hematuria is simply the medical term that doctors use for blood in the urine. Hematuria has multiple causes, and all causes of blood in the urine need to be evaluated by a urologist. Blood is divided into three broad categories: gross hematuria, microscopic hematuria, and dipstick positive hemoglobinuria.
There are other causes of colored urine besides blood.
Multiple foods, medications, medical conditions, as well as dehydration, can change the color of your urine.
The color and the odor of one’s urine are the most obvious characteristics to lay-people. Doctors are more concerned about how this relates to a microscopic evaluation of the urine for evidence of infection, stones, or cancer. Odor alone is rarely a first sign of urinary infection but most often is of little meaning if no other symptoms, such as pain, burning on urination, or frequent urination, are present.
The color of the urine is most commonly associates with the person’s state of hydration/dehydration. A well-hydrated person’s urine will be almost colorless while significantly dehydrated urine will have a very dark almost orange color. Dehydration is caused by not drinking enough fluid as well as by increased loss of fluid from sweating, diuretics, vomiting, and diarrhea.
The color of urine is affected by dehydration, foods such as asparagus, and by medications such as AZO, Pyridium or Phenazopyridine, and methylene blue for urinary pain. Multiple medications and foods can also change the color of your urine. Beets, which contain betalain, rhubarb, and blackberries will often change the urine to a pink or red color.
Urine color may be a sign of illness. Blood changes the urine red if the bleeding is fresh, but slow bleeding may change the urine to coffee, tea, or Coke-colored brown. Brownish urine my also be caused by fava beans and sometimes rhubarb. Liver disease such as hepatitis may make the urine a very dark yellow to brownish tint. Beta-carotene from carrots and supplements and high-dose vitamin C may cause the urine to be orange. In some people, the consumption of high-dose B vitamins and asparagus may occasionally turn the urine green.
Odor of urine is affected by medications and foods. Asparagus causes some people’s urine to have a strong odor. Urinary infection may be associated with a change in urine odor. Antibiotics frequently change the odor of urine. Diabetes is said to give the urine a sweet smell. Dehydration and some infections increase the amount of ammonia smell in the urine.
Urine can be red, orange, yellow, green, blue, indigo, violet, white, or black.
For a full list of foods, medications, and medical conditions that may change the color of your urine, scroll to the bottom of this page.
Back to hematuria:
The initial test on urine done by all doctors’ offices is the chemical dipstick test. This is a plastic stick with small pads attached. Each pad is impregnated with a different chemical. These pads change color in the presence of the substance they are specified to detect. They look for blood, pus, protein, nitrite, and several other factors commonly found in urine. The darker the shade the indicator color turns the more of that substance there is in the urine.
Gross hematuria is the most bothersome to both the patient and the urologist. It takes very little blood to turn the urine red. Seeing a little, red urine is enough to see the urologist. Even seeing the redness once is enough to see a urologist. This is not, however, an emergency. You do not normally need to go to the emergency room or call the doctor after hours.
Microscopic hematuria is usually found by a chemical dipstick and further evaluated in the laboratory by a microscopic examination of the urine confirming the presence of visible red blood cells (RBCs). Normal centrifuged and concentrated urine will have 0-3 RBCs per high-powered microscopic field (HPF). The centrifuged drop of urine is usually viewed at 400 power magnification. More RBCs than 0-3 need an evaluation.
Dipstick positive hematuria or hemoglobinuria is found on chemical testing, but there is no corresponding increase in number of RBCs found on microscopic examination. This is because dissolved hemoglobin is found by the chemical dipstick. This is a color change test. The yellow pad on the dipstick turns to progressively darker shades of green in the presence of hemoglobin or blood. It is currently thought that the filtration process in the kidney is breaking open RBCs, and the internal hemoglobin is released and dissolves. If there is no associated protein increase in the urine or if there is a history of difficult to control hypertension, monitoring this alone with serial microscopic urinalyses is all that is needed. If the hematuria is associated with proteinuria and hypertension, it may need to be evaluated by the medical kidney doctor, the nephrologist. Hemoglobinuria is found in about 5% of the adult population.
Evaluation
Dipstick positive hematuria:
Unless this is associated with malignant hypertension and more than a trace of protein in the urine, there is usually no cause for alarm. Dipstick positive hemoglobinuria simply needs monitoring. Usually this monitoring will be for a period of two to three years and all that’s needed is periodic visits to the urologist’s office for a simple, painless microscopic RBC evaluation. We like to refer to this visit as your “pee in a cup” visit. Repeating the microscopic urinalysis is all you may be asked to do. Unless associated with some other urologic problem such as recurrent infections, stones, or history of bladder problems, no cystoscopy or CT scan is usually required. Heavy protein associated with severe hypertension may be a sign of kidney disease. These people may need to see the nephrologist. The nephrologist is the medical kidney doctor. Urologists are the surgical kidney doctors.
Gross and Microscopic Hematuria evaluation:
Many things can put blood in the urine. While the most common things are benign, there are some cancers of the urinary tract that must be ruled out. Initial evaluation consists of an x-ray, a visual inspection of the bladder, and possibly some urine tests. X-ray examinations of the upper urinary tract can be accomplished with a CT urogram or an intravenous pyelogram (IVP). Both are used to look for stones, birth defects, and cancers of the kidneys and ureters.
The visual examination of the bladder is called a cystoscopy. This is required to look for polyps, stones, infections, prostatic bleeding, and cancer of the bladder. After introduction of Lidocaine anesthetic gel into the urethra in men or applied to the scope in women, the telescope is inserted into the bladder. This is not the rigid metal 7 millimeter telescope of the 1980s. The telescope has been flexible for many years now. The Flexible scope is a 5 millimeter scope. The average catheter inserted at surgery or on hospital admission is 5.3 to 6mm. Cystoscopy is a telescopic evaluation done in the urologist’s office. A thin, flexible telescope is guided through the urethra into the bladder. In men, both the prostate and the bladder are inspected. Inspection usually takes less than 2-3 minutes. The bladder is lined by mucosa. The lining looks much like the inside of the oral cavity or eyelid. Abnormalities as small as 2-3mm are easily seen.
Some burning on urination following the cystoscopy may occur. This usually lasts for 2-3 urinations. The urine infection rate from simple out-patient cystoscopy is about 1%. On occasion, you may see blood in the urine for less than a day. If the burning lasts more than 24 hours, you should call your urologist. You may be infected.
Urine tests for cancer such as a visual Pap smear of the urine or urinary cytology may be ordered. Several other chemical markers are also available but may not be needed. These include Nuclear Matrix Protein #22 (NMP-22) and FISH assay (fluorescence in situ hybridization).
Follow-Up
Long-term follow-up for up to 3 years is recommended if the initial evaluation is negative. This usually consists of repeated microscopic urinalyses in the office but may require repeat X-rays in some patients. If the number of RBCs increases on serial urinalyses over time, there may be something in the urinary tract that was too small to find the first time around. In this case, the x-rays and cystoscopy may need to be repeated.
Causes of Hematuria
There are multiple causes of blood in the urine. They range from urinary stone disease (stones in the kidney, ureter, and bladder) to prostatic problems to infections. All of the above are far more common than cancers of the kidney, bladder, and prostate, which most patients are worried about. All people with blood in their urine should be evaluated by a urologist as soon as symptoms present.
Foods, Medications, and Medical Conditions that may change the color of your urine
cresol, some plastics
hemolytic anemia
Melanoma, metastasis to the urinary tract
porphyria
Blue green urine from medication
amitriptyline, Elavil
cimetadine, Tagamet
Flupirtine
indigo carmine
Indomethacin, Indocin
metaclopromide, Reglan
methylene blue
phenol, throat spray, EU not USA
promethazine, Phenergan
Propofol, anesthetic
triampterine, diutetic
Zalepon, insomnia
Foods that turn urine blue green
Asparagus
black licorice
Blue dye #1, food coloring
Clorets breath mints
Medical conditions blue, green
Biliverdin
Hartnup disease
herbicide ingestion
porphyuria
pseudomonas UTI
pseudomonas UTI, blue diaper synd
tetrahydronaphthalene
tryptophan, abnl metabolsim with UTI
Purple, blue urine
Blue diaper syndrome is the same, similar
Gram negative UTI, indole metabolism may
porphuria when exposed to sunlight
pseudomonas, UTI
turn the catheter tubing blue
White Urine
Albuminuria, proteinuria
Calcium phosphate cyrstals, normal
Chyluria, lymphatic fluid in the urine
Filariasis
Funguria, yeast infection, candidiasis
Lipiduria, fat, cholesterol, trigycerides
lymphatic fistula
mineral sediment hypercalcuria
mineral sediment hyperoxaluria
mineral sediment phosphatuira
mycobacturia, Tuberculosis
propophol infusion
puyria, infection, pus
schistosomiasis
Urinary tuberculosis
Urinary Tract Infections (commonly referred to as UTIs) are very common infections. We see more women than men for UTIs because about 40 % of women and only 12% of men will develop UTIs. (Men instead develop prostatitis, which is covered in another section.)
Urine infections in women have several names. They are essentially all describing the same thing, an infection of the bladder. The most correct term is cystitis, an infection of the bladder. These are confined to the bladder and do not ascend up the ureter to the kidneys. They are also called urine infection, bladder infection, kidney infection, and urinary tract infection (UTI).
UTI is a broad term that does not specifically single out the site of the infection. Urethritis is an infection of the urethra. The urethra is the tube from the bladder to the outside of the body.
Cystitis is the true term for an infection of the bladder.
Normal Female Urinary Tract
Prostatitis is an infection of the male prostate gland. Women do not have a prostate.
Ureteritis is an infection of the ureter. This is the tube that connects the kidney to the bladder.
Pyelonephritis is a true infection of the kidney. The initial bladder infection has gained access to the ureter and traveled up all the way into the kidneys.
Urosepsis or “blood poisoning” is an infection that has invaded into the blood stream.
Symptoms of UTI
Frequency of urination suddenly increases.
Urgency is the sudden urge to get to the toilet for fear of incontinence.
Dysuria is that burning sensation that occurs with urination.
Nocturia is the need to get up in the night to urinate.
Hematuria is the finding of blood in the urine.
Pelvic pain occurs in women.
Rectal pain may be found in men.
Cloudy urine may be a sign of infection.
Persistent urge to urinate and a feeling of fullness after urination may be present.
Strong odor to the urine may develop.
Feelings of incomplete emptying are common.
Incontinence of urine is found in some people.
Painful sex occurs in women.
Painful ejaculation occurs in men.
Low-grade fever < 100°F for cystitis. High fever >101°F, with chills, nausea, and vomiting in pyelonephritis.
Elderly people may have loss of appetite and occasional mental changes or confusion.
Causes of UTI(s)
Women have several times in their life where the risk of a UTI is known to increase.
The first time for females to acquire a UTI is as a child. Children with UTIs usually need an evaluation for birth defects of the urinary system. The most common defect is ureterovesical reflux. In this situation, the insertion point of the ureter into the bladder is abnormal, and urine flows backwards into the kidney during urination. This backward or retrograde flow is called reflux.
Kidney, Acute Pyelonephritis
The second time in a young woman’s life that the number of UTIs increases is with the onset of her menstrual cycle. Whether this is due to tampons and pads or hormonal changes, it is not clear.
Onset of intercourse has long been noted to cause a UTI in women. That is where the term ‘honeymoon cystitis’ comes from. Due to the position of the female urethra in the upper edge of the vagina, sex irritates the urethra and allows bacteria to enter the urethra. Since the urethra is shorter in women than men, it is easier for the bacteria to ascend into the bladder. In most women, cystitis occurs a few times and goes away. In a few cases, intercourse remains a frequent source of UTIs throughout her lifetime.
Kidney, Chronic Pyelonephritis
Pregnancy is noted to have an increased incidence of UTIs in some women. Whether this is hormonal, immunosuppression in the mother, or stasis in the system, it is not clear. The gravid or pregnant uterus begins to compress both ureters at about 20 weeks. This compression first affects the right kidney, and then a few weeks later it affects the left side. The pressure of the enlarged uterus upon the ureters at the pelvic brim creates hydronephrosis or back up on both kidneys.
Menopause is also noted to bring on an increase in frequency of UTIs. The degree of difficulty of treatment increases as well. The loss of estrogen has a direct effect on the health of the lining of the bladder as well as the lining of the vagina.
Evaluation
Evaluation for repeated UTIs is advised in women having more than 4 per year, one that will not clear, or with pyelonephritis.
Evaluation will include:
Urinalysis is done to see if the symptoms are truly a UTI. Some of the other illnesses that may mimic UTIs are interstitial cystitis (IC), estrogen deficiency, and endometriosis.
Urine cultures may be sent to the laboratory. The urine is set up to see if a bacteria grows and how many. If bacteria grow, then they are treated with different antibiotics to see which one is the most effective treatment.
The post-void residual urine will be checked to make sure the bladder is empty. Poor emptying leads to repeated UTIs that are difficult to clear. The difficulty in clearing the UTI is due to the stagnant urine left in the bladder after each urination.
Ultrasound or bladder scan measurement of this residual urine is non-invasive and does not require a catheter be inserted into the urethra.
Pelvic exam looks for cystocele formation, descent of the bladder into the vagina after childbirth.
X-ray evaluation such as renal ultrasound, intravenous pyelogram (IVP), or CT urogram may be ordered to evaluate for obstruction of the ureters, signs if old scarring from childhood reflux, stones and/or tumors.
Cystoscopy is used to evaluate the lining of the bladder. Flexible cystoscopes are used in the office and are more comfortable than rigid cystoscopic evaluations.
Treatment
Common Antibiotics for treatment are:
Sulfa/ Bactrim/ Sulfamethoxazole and Trimethoprim
Ampicillin or Amoxicillin
Cipro or Levaquin
Doxycycline
Trimethoprim
Cephalosporins/ Keflex
Nitrofurantoin/ Macrodantin/ Macrobid
Prevention of UTIs
The vast majority of young girls are taught to wipe urine and stool from front to back. This is to prevent the bacteria around the anus from being brought forward towards the vagina. The perineum is that area behind the vaginal opening and includes that area in front of the anus. The most common bacteria to cause a UTI are the enteric bacteria that grow on the perineum. Proper hygiene is the first line of defense against infections.
Anything that might irritate the vaginal area may lead to infections. Bubble baths in small children as well as perfumes, feminine hygiene sprays, and laundry detergents have been implicated. The irritated skin is more prone to bacterial colonization. The increased density of bacteria in that area leads to more opportunities for the bacteria to get into the bladder.
Since intercourse is a common time for bacteria to enter the urinary tract, it is advised that women wash before intercourse. Washing after intercourse may lower the infection rate by removing lubricant, bacteria, and semen. Urinating after intercourse should empty out any bacteria that entered the urethra. This helps to get rid of the bacteria before they have a chance to grow into an infection. In rare occasions, your doctor may give you an antibiotic to keep on hand to be taken immediately after intercourse. Usually a single dose of antibiotic will do in this situation. This single dose of antibiotic lowers the risk of yeast infection as well as any interference that antibiotics may cause with your birth control pills. Longer courses of antibiotics may lower the effectiveness of birth control pills.
Some studies show that there is an increase in bacterial adherence to the vaginal mucosa with changes in the hormones at different times in the menstrual cycle. Many women have told me that only at certain points in their cycle are they susceptible to UTIs with intercourse. Please tell your urologist if you have found a pattern to your UTIs.
Women also say that there is a difference in a UTI risk based on sexual position.
Some women relate the risk of a UTI to whether they use tampons versus pads. Usually, as long as they are changed regularly, it should not make a difference.
Estrogen deficiency after menopause leads to vaginal dryness. This in turn leads to better adherence of bacteria to the skin and vaginal lining with increased risk of a UTI. The normal vaginal moisture contains factors that help prevent UTIs. Without this moisture and its antibodies, infections may increase in both number and severity. After stopping estrogen replacement therapy, there is an increase in UTIs.
Incontinence leads to skin irritation and an increased risk of a UTI. This is likely due to the ammonia irritation of the skin with increased bacterial colonization.
Cystoceles, also called prolapsed or dropped bladders, often occur after childbirth. The leftover urine increases in the bladder as the cystocele increases in size. This stagnant urine leads to an increased risk of a UTI.
Diabetics have a decrease in their ability to fight infection and develop more frequent UTIs. Good control of your diabetes will reduce your UTI risk.
Cotton panties absorb moisture better than nylon and may reduce your UTI risk.
Water based lubricants work better than petroleum or silicone based lubricants for prevention of UTIs.
Don’t douche. Douching washes away any protective factor that the normal vaginal secretions provide in preventing infection.
Tight clothing such as tight jeans and pantyhose has been implicated.
Do not continue to wear sweaty gym cloths any longer than necessary.
Drink plenty of water.
Spermicides alone or on condoms may cause UTIs.
Diaphragm usage has been noted to increase the risk of UTIs more than other forms of birth control.
Constipation may increase UTIs especially in children and the women of advanced age.
An uncircumcised sex partner leads to an increased risk for getting UTIs. An unclean foreskin will harbor bacteria which can be transferred to the urethra.
Most Common Bacteria
These are the bacteria that normally live on the perineum. They are called enteric bacteria and are normal in the colon. E.coli is the most common of all bacteria to cause a UTI. E.coli accounts for 80 to 85% of uncomplicated UTIs. Other organisms include Klebsiella, Serratia, Providencia, Proteus, Enterococcus, Enterobacter, Pseudomonas, Staphylococcus, and Streptococcus.
Diagnosis
Urinalysis is the initial test for a UTI diagnosis. This begins with a chemical dipstick that changes color in the presence of blood, bacteria, and white blood cells (WBCs). These dipstick test results can be falsely positive if there is contamination from the urine flowing past the vagina. False positives also occur with yeast infections.
Microscopic urinalysis consists of placing 10-15cc of urine in a centrifuge for 10 minutes. The liquid is poured off, and the last drop is resuspended and placed on a microscope slide. Under 400-power magnification, the urine undergoes a white blood cell count (WBC), a red blood cell count (RBC), and an evaluation for crystals, bacteria, and epithelial cells. Epithelial cells are a sign of vaginal contamination and may invalidate a positive dipstick urinalysis.
Cultures are used to grow the bacteria in the laboratory under controlled conditions. If bacteria grow, then they are tested against antibiotics to determine the sensitivity of the bacteria. The bacteria are tested against multiple antibiotics. If serial cultures show the same bacteria over and over again, then it is thought that the original UTI has never cleared. If there are different bacteria on successive cultures, then it is felt that this is most likely a repeat infection. Multiple organisms indicate vaginal contamination. Lactobacillus is also felt to be due to vaginal contamination. Beta Strep is a normal perineal and vaginal bacterium and may be contamination, not a UTI. A positive culture from a voided specimen should contain 10 to the 5th power of colony forming units of a singe organism. Multiple organisms call into question that the specimen was contaminated and not a valid specimen. Catheterized specimens are positive at 10 to the 4th power CFU (colony-forming unit).
Specimen Collection
A voided urine specimen is obtained if possible. This is to try to avoid obtaining a catheterized specimen. Catheterization is the introduction of a small tube up the urethra into the bladder just far enough to get a urine specimen. Catheterization does avoid the risk of contamination.
A voided specimen may be obtained. While most women just urinate in a cup without proper cleaning, this is the worst possible specimen for accurate diagnosis. A proper specimen starts by cleaning with the antiseptic towelette. Cleaning should be all the way to the vaginal opening. With one hand, the vaginal lips or labia are held apart, and the cup is held in the other hand. A small spurt of urine will then wash away any lingering contamination. The midstream 2-3 ounces of urine are then caught in the specimen cup, with the remaining urine voided into the toilet.
UTI Treatment
The treatment of the UTI depends on whether it is classified as complicated or uncomplicated. An uncomplicated UTI is a simple bladder infection without fever or association with stones, catheters, or other complicating illnesses.
A complicated UTI is associated with fever >101°F, infection behind an obstructing kidney stone, or an infected catheter.
An uncomplicated UTI is treated with oral antibiotics. In young, healthy, college coed’s, studies have shown that 50% will clear with one dose of antibiotics. The problem is that 100% burned on urination or had other symptoms for 3 days. So therapy in healthy individuals should be limited to 3 days. If the woman has incomplete emptying, a history of failing to clear in 3 days, is diabetic or estrogen deficient, or is on immunosuppressant drugs, the treatment may be 5-7-10 or even 14 days.
A complicated UTI usually requires hospital admission with IV antibiotics. If associated with a kidney stone, the kidney will need to be unblocked before antibiotics can be effective.
Other Medications
Pyridium or Phenazopyridine is an AZO dye, that when excreted in the urine, acts as a topical anesthetic.
Methylene blue is a similar dye for topical anesthesia.
Antispasmodics or anticholinergic medications used for overactive bladder are also effective in treating the bladder spasms so often associated with a UTI. These help with the frequency and urgency of urination until the antibiotic can kill the bacteria. Brand names are VESIcare, Enablex, Toviaz, Ditropan, Levbid, and Detrol.
Home Remedy
Drinking plenty of fluids will increase urine production and may flush out the bacteria, but rarely will your body be able to clear the infection.
Cranberry juice and tablets are reported to help treat and prevent a UTI. One study reported that if one drank 32 ounces of cranberry juice per day, there was a 20% reduction in the number of UTIs. That means if a woman has 5 UTIs per year the cranberry juice lowered that number from 5 to 4. Most people do not drink 32 oz of fluids per day in the first place. High intake of cranberry juice may cause kidney stones.
Taking a warm tub bath may relax the bladder spasms.
Ibuprofen and other NSAID medications are anti-inflammatory medications and may help relieve the pain of urination.
AZO over the counter is the same medication that is in prescription strength Pyridium. The dose has been reduced only from prescription strength 100mg to 95mg in the AZO over the counter.
Reports that pineapple juice relieves UTI symptoms are based on its purported anti-inflammatory effects on the bladder.
Difficulty in conceiving a child is called infertility. Infertility is different than sterility. Sterility refers to the conditions that totally prevent pregnancy from occurring. The medical definition of infertility is the inability for normal people to get pregnant after one year of stopping birth control. This article is here to discuss conditions in men that contribute to problems with conception.
Infertility is a complex medical problem and can occur due to both male and female factors. Men alone account for about 30% of infertility. In an additional 20% of infertile couples, there is a combination of both male and female factors contributing to problems with conception of a child.
Infertility is a problem for 15-20% of all couples in the USA. This equates to between 4 and 5 million men in the USA. With modern technology, many causes of infertility are now treatable.
In addition, over the last 4-5 decades, there has been a slow, worldwide decrease in the number of sperm with normal morphology emitted per ejaculation. The cause of this is unknown but is theorized to be due to the number of chemical pollutants in the environment. Examples of these chemicals are DDT, dioxin, polychlorinated biphenyls (PCBs), and hexachlorobenzene. While some of these chemicals are toxic, many of these chemicals act as estrogen-like compounds.
Men taking estrogen have a decrease in sperm and testosterone production. Foods such as soy products are high in isoflavones. Isoflavones are in the category of phytoestrogens. Phytoestrogens are estrogens in plants that may affect hormone levels in humans.
An alternate theory is that the epidemic of obesity plays a significant role in declining fertility. Obesity has been directly tied to diabetes. Diabetes has several effects on men. Obesity is associated with both erectile dysfunction (ED) and an increase in circulating estrogen. Both of these conditions contribute to infertility.
Infertility Evaluation Costs
Infertility treatment costs are frequently not covered by health insurance. That does not mean that the basic evaluation is not covered under your health insurance policy. Infertility treatments such as In Vitro Fertilization (IVF) and Intra Cytoplasmic Sperm Injection (ICSI) can run into the tens of thousands of dollars. These two treatments are what are usually not covered by regular health insurance policies.
If your semen quality can be optimized to a sperm count of 20 million, you may want to look for a gynecologist that does artificial insemination. This usually costs about $1,000 per cycle, and most couples will achieve pregnancy in 4 cycles. This is much cheaper than even one cycle of In Vitro Fertilization (IVF). It seems that most of our local fertility clinics do not find artificial insemination cost effective enough for them to perform, and they have stopped offering artificial insemination. Instead, they immediately opt for the more expensive and higher tech therapies of IVF and ICSI.
On the other hand, a basic evaluation may only be a couple of thousand dollars. Frequently, your insurance will cover the cost of the basic medical tests. If you shop around, the evaluation can be done one step at the time. Stopping the testing, when the evaluation identifies a treatable cause of male infertility, allows for treatment of that cause of infertility. After appropriately 3 months of treatment, re-checking a semen analysis will then evaluate your response to that therapy.
Be patient. Men can only be cycled on a 3 month basis. It can be a several, month long process to identify and improve male infertility. Most treatments show an improvement rate of about 30% at three months of therapy. So, as you see, your urologist may need to try 3-4 different treatments over 12 months before finding something to which you may respond.
While many men are embarrassed about discussing their problems with their urologist, it is important to give a complete history of any symptoms you may have. This will help your urologist determine which tests are covered by your insurance policy and which are your responsibility. That way, there are no hidden costs for you later. If you have erectile dysfunction (ED), decreased libido (Low T), fatigue, decreased energy levels, decreased stamina at sports, weight gain, or memory problems, your labs may be covered by your basic health insurance. This would possibly include all the basic blood work such as testosterone, FSH, LH, prolactin, thyroid function, and all basic chemistries.
If you have a varicocele on physical examination that is associated with testicular pain or small testicular size, insurance should cover the cost of a scrotal ultrasound. At an imaging center, not a hospital, this ultrasound may cost anywhere from 1/10th to 1/5th of the hospital cost for the same ultrasound. For example, at an imaging center, the cash price locally is about $250 (3/1/2013). At an imaging center, you may pay an office co-pay rather than the hospital deductible, which can be anywhere from $500-$5,000 depending on your policy. An imaging center’s lower price is a cash-only, one-time sum; they do not have payment plans. You may need to shop for the best price yourself; many offices don’t seem to know the out of pocket patient costs of the tests they order.
A semen analysis is rarely covered by health insurance. Not many hospitals continue to do this test. The basic cash price is currently about $150-$200. (3-1-2013)
Once you have been billed for a service through your insurance, if it is not a covered service, then you are responsible for the full price of the lab tests. Therefore, at the time of your initial visit, ask your doctor about his wholesale lab account, if he has one, and what it would cost you to pay him cash up front for the tests versus your insurance cost. Your doctor’s cost is about 25-30% of your cost if the labs are billed to his commercial account. If rejected by your insurance, this cannot be rebilled to the doctor’s account at a later time. For example, a total and free testosterone is currently about $45 through the wholesale account, but billed through the lab to you, you would be responsible for roughly $145. Most doctors will need for you to pay this up front; they do not have laboratory payment plans. This arrangement still saves you a lot of money.
Beginning an infertility evaluation may seem like an overwhelming task, but taken a step at the time, the evaluation can be accomplished at an affordable rate for most couples.
Possible Reversable Causes of Infertility
Your urologist will take a full history to help look for the most easily treated causes of infertility. Infertile couples can make some lifestyle changes and decrease their degree of infertility.
Men trying to conceive may want to consider these changes in advance of trying to conceive. It will likely take up to 3 months after cessation of the use of drugs, tobacco, and alcohol before semen quality improves.
Smoking cessation helps improve semen quality. Tobacco usage causes problems with sperm motility. The decrease is in the range of a 10-15% decrease in motility. Motility is the medical term for the sperm’s ability to swim in a straight line, also described as forward progression. Tobacco has also been linked to sperm death. There is a 20-25% decrease in sperm concentrations in men that smoke. Smoking also causes DNA damage within the sperm’s chromosomes, resulting in larger numbers of damaged sperm. DNA damage is theoretically due to the cadmium found in cigarette smoke replacing zinc in DNA polymerase.
Caffeine intake has been noted in some studies to decrease sperm motility as much as 20-30%. Therefore, a reduction in caffeine may be beneficial.
Marijuana smoke has been shown to have a similar effect as that of tobacco on sperm movement or motility. Abnormal sperm and increased numbers of dead sperm are noted on semen analyses of chronic smokers of marijuana. Marijuana use, unlike tobacco use, also has the reported effect of lowering testosterone levels. Low testosterone results in lower sperm counts. When the abnormal sperm do result in fertilization, there is an increased risk of miscarriage.
Alcoholcan have multiple effects on sperm as well. Alcohol affects testosterone levels. Alcohol effects on the liver result in an increase in men’s estrogen levels. Increased estrogen levels counterbalance testosterone levels. Regular intake of more than 3-4 beers per night or 2 drinks per night containing 1 ounce of alcohol per drink is enough to affect semen quality. Binge drinking even one weekend a month likely has the same effect as daily drinking.
Recreational use of Cocaine, Heroin, PCP and amphetamines has been linked to infertility. Cocaine increases the number of abnormal sperm, decreases sperm counts, and causes a decrease in sperm motility. Cocaine has been found to decrease the sperm’s ability to penetrate cervical mucus. Cocaine enters the testicular tissue and attaches to the sperm. Cocaine then enters the egg reportedly increasing the risk of birth defects. Cocaine and heroin users may have abnormal semen analyses as long as 2 years after their last use of the drug. All of these drugs have an association with ejaculatory dysfunction, erectile dysfunction, and decreased sex drive or libido.
Chronic use of narcotics (opioid medications) for pain may lower testosterone levels. This includes both legal and illegal narcotics. Percocet (Oxycodone), Vicodin (Hydrocodone), and Demerol (Meperidine) are examples of these types of medications.
Men quite commonly use anabolic steroids. Some studies suggest that 5-6% of 18-year olds have tried or regularly use steroids as a body building aid. These drugs can permanently damage the testes and their ability to make sperm or testosterone even after the steroids are stopped. Sperm counts may return to normal 4-12 months after stopping anabolic steroids.
Avoiding heat to the scrotum helps restore sperm numbers and motility. Heating the scrotum to 101°-102°F has a significant effect on sperm quality. Sperm quality may be improved by avoiding hot showers, hot tub baths, and constrictive clothing. Wearing tight jeans and other constrictive clothing does not allow the testicles to drop away from the body when they are hot. Increased heat damages sperm and sperm producing cells in the testicle. The scrotal skin elongates when men are hot. This helps regulate the temperature of the testes. Even prolonged periods of time above 98.6°F may damage the testicles. Saunas have the same affect on sperm viability and motility as hot baths and showers. Laptop computers have been shown generate enough heat to affect sperm quality. Tanning bed sessions may also affect semen parameters.
Timing of intercourse is helpful in conceiving a child. There are only 3-5 days in a woman’s cycle when the egg is available for fertilization. Having intercourse every other day during this time may deposit sperm in higher concentrations in the vagina than daily intercourse deposits. Abstaining from intercourse for 4-5 days before your partner ovulates also helps increase the sperm density. Intercourse less often than 10-14 days may decrease sperm motility.
Heavy exertion such as training for a marathon or triathlon has been observed to decrease semen quality.
Medications Affecting Fertility in Men
There are a number of common medications that may interfere with hormone levels, be toxic to sperm, or interfere with fertilization. A partial list and their use are as follows:
Lubricants such as lotions, KY jelly, Astroglide, petroleum jelly, and saliva have been shown to kill sperm. These should be avoided.
Hypertension or high blood pressure is often treated with the following medications. (Please do not stop these medications without your primary doctor’s help in switching to a different medication.)
Calcium channel blockers like Calan (verapamil), Cardizem (diltiazem), Norvasc (amlodipine)
Beta blockers include most medications ending in “olol”. Atenolol is and example.
Alpha blockers may be used for hypertension or prostate issues. Flomax (tamsulosin) etc.
Thiazide diuretics are sued in hypertension control. Hydrochlorothiazide (HCTZ)
Spironolactone is a potassium sparing diuretic.
Reserpine
Estrogen: phytoestrogens in the diet and estrogens in prescription medications.
Progesterone
Ketoconazole is an antifungal medication that lowers testosterone.
Antiandrogens are most commonly used in the treatment of prostate cancer: Casodex (Bicalutamide) and Eulexin (Flutamide).
5-alpha-reductase medications for benign prostatic hypertrophy may lower hormone levels in some patients; these include Proscar (Finasteride) and Avodart (Dutasteride).
Tagamet (cimetidine) lowers testosterone levels.
Antidepressants in many different classes may cause problems. These problems include both decreases in libido or sex drive and ejaculatory problems.
SSRI or Selective Serotonin Reuptake Inhibitors: Celexa (Citalopram), Lexapro (Escitalopram), Prozac (Fluoxetine), Paxil (Paroxetine), and Zoloft (Sertraline) have been associated with erectile dysfunction (ED), decreased sex drive (libido), and lack of orgasm or anorgasmia. Due to a side affect of difficulty ejaculating, these medications have been used with some effect on premature ejaculation.
Tricyclic antidepressants such as Elavil (Amitriptyline), Tofranil (Imipramine), Sinequan (Doxepin), and Pamelor (Nortiptyline) as are most frequently used in chronic pain or insomnia.
Antibiotics that affect sperm are Erythromycin and Tetracycline. These antibiotics are used in dermatology and urology while Nitrofurantoin is only used for urinary infections.
Minocycline may be toxic to sperm.
Methotrexate is used for arthritis, cancer, or psoriasis.
Chemotherapeutic agents are frequently toxic to sperm production. This is frequently permanent.
Allopurinol and Colchicine, commonly used for gout, may interfere with fertilization.
Cyclosporine and Sulfasalazine are used as immune system suppressants in chronic inflammation inducing diseases.
Medications affecting testosteronelevels include:
Testosterone replacement therapy: topical gels (AndroGel, Axiron, Fortesta, and Testim), intramuscular injections (testosterone cypionate and ethanate), transdermal patches (Androderm), and buccal mucosal patches (Striant). Most oral medications are no longer used in the USA because they pose a risk of liver dysfunction and cancer.
History of Infections and Infertility
Infections of the testis are called orchitis. Epididymitis is the infection of the epididymal gland. Occasionally, this is referred to as epididymo-orchitis since both conditions frequently occur simultaneously. Bacterial infections are caused by the same bacterial organisms as prostatitis. E.coli is the most common organism. These infections may result in blockage of the vas deferens and epididymis.
STDs or sexually transmitted diseases such as gonorrhea (Neisseria gonorrhoeae) and nonspecific urethritis (Chlamydia or Mycoplasma) can lead to the inflammation and later obstruction of the vas deferens or the tubules within the epididymis. This obstruction can occur even in asymptomatic infections. It is important to tell your urologist if you ever had any of these infections.
Genital Examination in Infertility
Your urologist will need to examine you for physical causes of infertility. The penis will be examined for the position of the urinary meatus. The meatus is the opening on the tip of the penis. Hypospadias is the birth defect where the meatus is under the head of the penis and is not on the tip. Hypospadias may interfere with proper deposition of semen deep enough into the vagina. Deposition of the semen outside or just barely inside the vagina may not be adequate for conception.
The testicular exam is to evaluate the testes for normal testicular size. About half the volume of each testis is from the cells producing the sperm and the other half is from cells producing testosterone. Small testicular size may be due to inadequate production of either sperm cells or testosterone. Small size may be from inadequate development in the womb, trauma damaging a testicle, or from prior surgery as a child. Having a mumps orchitis infection as a child may cause enough swelling within the testicle to kill some of the cells inside that testicle. Trauma and rarely infection can have similar results.
Examination of the spermatic cord structures refers to the evaluation of the muscle, blood vessels, and vas deferens above the testicle up to its disappearance into the abdomen.
Varicocele is the medical term for varicose veins of the spermatic cord. The non-medical description of this is that the scrotum feels and sometimes looks like a “bag of worms”. This condition is more common on the left side but may be bilateral. Usually, there is an 80/20 ratio of left to right varicoceles. It may or may not cause pain after lifting or with long-term standing. It is occasionally associated with a decrease in the size of the testicle on the affected side. The veins are most prominent when standing and almost immediately flatten upon lying down. Repair consists of dividing (cutting) all these veins into. The best approach to these veins is where the veins exit the abdomen (internal inguinal ring) but before they reach the scrotum (external inguinal ring). Division of these veins usually increases sperm count and motility.
The vas deferentia are the tubes from the testes that carry the sperm up to the prostate. Your semen is a combination of the fluids produced in the prostate, seminal vesicles, and testicles. Ejaculation is the discharge of semen at orgasm. The scrotal examination will evaluate the vas deferens. The vas deferens or vas may be congenitally absent in families that carry the gene for cystic fibrosis. The vas can be damaged in childhood surgeries for hernia, hydrocele, and undescended testis. In the condition of undescended testis, the testicle is up in the groin and must be surgically placed into the scrotum. The most common damage is a crush injury that scars the vas closed. However, just the fact that the testis is undescended has an affect on the fertility of that testicle. Often, these testicles have a long, looped vas deferens with an abnormal insertion into the epididymis. Usually, the epididymis is abnormally attached to the testis.
The epididymis is the gland behind the testicle in the scrotum. The epididymis is adherent to the testicle. This gland is soft enough that most men do not know it even exists. The epididymis is the gland in which the sperm mature before traveling up the vas deferens. Enlargement may be an indication that the vas is obstructed. Cysts occasionally form in the epididymis as well. These are defined as simple cysts if they contain clear fluid. Those cysts containing sperm are called spermatoceles.
The prostate examination is a digital rectal examination (DRE). The urologist will check for signs of enlargement or infection of the prostate. Infected prostate glands are often soft or boggy feeling. Normally, little fluid can be expressed from the prostate. If a moderate or large amount of fluid is produced upon massaging the prostate, this fluid is then placed on a microscope slide for visual inspection for white blood cells (WBCs). WBCs secrete chemicals in their attempt to fight an infection. These chemicals may harm the sperm resulting in death or decreased motility. Clearing of the infection may resolve some infertility issues. The urologist usually cannot feel the seminal vesicles unless they are markedly abnormal. Occasionally, people that carry the cystic fibrosis gene do not develop seminal vesicles and vas deferens, and there is no way for the testis to add sperm to the semen.
Tests for Infertility
Blood tests and semen analyses are used to look for causes of infertility. The blood tests are to check for hormonal abnormalities. If the semen analysis has more than 10 million sperm, these tests are usually not necessary. The usual hormones evaluated are testosterone, total and free testosterone, and sex hormone binding globulin levels. These levels look for testosterone production from the testis. The Pituitary hormones involved are follicular stimulating hormone or FSH and luteinizing hormone or LH. FSH stimulates sperm production, and LH is involved in testosterone production.
If the testosterone level is low, additional tests for prolactin levels and thyroid hormones may be needed.
Measurement of blood sugar or blood glucose and hemoglobin A1C may be needed to check for diabetes or to check one’s level of diabetes control.
Semen analysis is the direct microscopic evaluation of the ejaculated semen. This looks at multiple different parameters.
Semen Collection for Analysis
Masturbation is the most accepted form of collection. This normally produces the most complete specimen. Specimens from condoms are much less useful. These contain many skin cells lost from the skin surface during intercourse. Unless a special condom without spermicide is used, the spermicide will kill the sperm. Collection condoms are made of silicone or polyurethane since latex is toxic to sperm. There is no way to determine if the sperm died from spermicide exposure or if the sperm were dead at the time of ejaculation. If coitus interruptus is used and even a small amount of the ejaculate is lost, the test results will be artificially abnormal. The use of any lubricants or saliva will also kill the sperm.
Transportation of the specimen is best done at body temperature. Placing it in a shirt pocket or between the thighs is the easiest way to achieve this temperature. Sperm begin to die within an hour of ejaculation. If the specimen is brought to the laboratory within 20-25 minutes, the appropriate tests can begin before that hour has elapsed. Sperm begin to die, in a specimen cup, at a rate of about 10% per hour after ejaculation.
Terminology of Semen Analysis
Oligospermia refers to a decreased number of sperm.
Aspermia is the total lack of semen.
Hypospermia is low sperm volume.
Azoospermia is the absence of sperm in the semen.
Teratospermiais an increase in sperm but they are morphologically abnormal.
Asthenospermia is reduced sperm motility or ability to swim.
Motility refers to the ability to swim.
Morphology refers to the normal or abnormal appearance of the sperm.
Vitality refers to the sperm being alive at the time of ejaculation.
Liquefaction measures the time it takes the semen to go from a gelatinous state to a liquid state.
Fructose is a type of sugar in the semen. It is chemically the same sugar found in fruit.
106 is scientific notation for 1 million.
Volume is the amount of semen produced measured in cubic centimeters or ccs.
Sperm Concentration is the number of sperm per cc or milliliter (ml).
Sperm count is the total number of sperm per ejaculation.
Motility is expressed as a percentage of how many of the sperm are moving.
Morphology evaluates the shape of the sperm.
Liquefaction looks at the time it takes semen to turn from a gel to a liquid.
Progression evaluates forward movement of motile sperm.
Vitality measures the percentage of sperm alive in the fresh specimen.
White Blood Cell Counts look for infection that may be affecting semen quality.
Agglutination is the clumping together of sperm.
Fructose should be present in the semen, and when fructose is absent, blockage is frequently present.
Inhibin B may be measured and low levels may indicate blockage.
Alpha-glucosidase levels, if found to be low, may also indicate blockage.
A post-ejaculatory urinalysis can be used to look for retrograde ejaculation. This is the medical condition where the semen goes back into the bladder rather than out the penis at the time of ejaculation. It occurs with diabetes, spinal injury, and some medications.
Interpretation of Semen Analysis
Your doctor doesn’t just read the numbers off of your semen analysis report; he must instead interpret the results. What the semen analysis shows is what is normal. This is different than what is adequate for conception.
An example of the difference in normal and adequate is that it is normal to have two kidneys, but one is adequate for a normal life. It is normal to have 10 fingers, but many people get along adequately after the loss of multiple fingers.
Due to a wide daily variation in semen analysis values, 2-3 specimens may be required to determine if a man is infertile.
Semen volume may be low if intercourse is too frequent, such as daily ejaculation.
Low volume may indicate obstruction, retrograde ejaculation or incomplete collection. In retrograde ejaculation, the sperm may be seen on a post-ejaculatory urinalysis.
A pH that is >8.0 may indicate a prostate infection. Low pH <7.2 may indicate blockage of the seminal vesicles. If fructose is also absent, the seminal vesicles are blocked.
Please note that in “normal” individuals’ normal-looking sperm or normal morphology is present at a level of only 30%. Alternately, 70% of the sperm in a normal specimen are abnormally formed and not able to fertilize an egg.
White Blood Cell (WBC) counts that are elevated have been found in up to 10-20% of men tested for infertility. WBCs are designed to kill bacteria. When present in semen, these WBCs can kill sperm as well. Immature sperm cells must be differentiated from WBCs as they look very similar. WBC counts also increase in men with sub-clinical prostatitis.
Motility may be low due to not ejaculating at least every 10-14 days or due to heat exposure: environmental or fever.
Fertility comes down to a game of numbers. All of the parameters in a semen analysis do not have to be normal for an individual man to be fertile.
Contrary to popular belief, one sperm and one egg do not usually result in fertilization. Under normal circumstances, it takes multiple sperm to break down the zona pellucida or outer coating of the human egg (ovum) before one sperm finally penetrates and fertilizes that egg.
Let’s start with an example of the numbers needed for successful intrauterine insemination.
What is said to be adequate for insemination is a semen specimen of 1 ml, containing 20 million sperm with 20% (0.20) normal motility and 20% (0.20) normal morphology.
This then equals 1 x 20 million x 0.20 motility x 0.20 morphology= 800,000 normal sperm.
So, if an individual has, for example, a specimen of 1.5 ml, a count of 18 million sperm/ml, an abnormal motility of 30% (0.30), and a low morphology of 20% (0.20), this appears to be quite abnormal. The math however is quite different.
This equals1.5 ml x 18 million x 0.30 motility x 0.20 morphology=1.6 million normalsperm. So while on the surface this specimen has multiple abnormal values, it is still possible to achieve pregnancy through insemination but not through intercourse. The increase in volume and motility, in this case, make up for the lower sperm count.
Using the lowest normal semen parameters of 20 million/ml x1.5 ml x 0.50 motility and 0.30 morphology=4.5 million normal sperm. While pregnancy is achievable at these semen analysis levels, conception will likely take timing of intercourse and up to 12 months or more to achieve pregnancy.
Pregnancies have been achieved at lower counts, but as the sperm count decreases, so does the chance of conception. It is rare that a man can achieve conception at sperm counts less than 10 million/ml even with all other parameters being normal. Unfortunately, most of the time, low sperm counts are associated with low motility as well. Even at mid range numbers such as 3 ml x 10 million/ml x 0.50 motility x 0.50 morphology=7.5 million normal sperm, this would be barely adequate for conception through intercourse.
Some studies suggest that sperm motility is more important than sperm concentration and sperm morphology. The lowest semen parameters that are adequate for readily achievable pregnancy through intercourse may be 10-12 million viable sperm.
Mid range normal values of a volume 2.5ml x 20 million/ml x 0.40 motility and 0.50 morphology =10 million normal sperm.
At counts around 15 million/ml, it is a little easier to reach adequate numbers of normal sperm; therefore, 15 million/ml x 3 ml x 0.50 motility x 0.50 morphology=11.25 million normal sperm.
Ultrasonic Evaluations for Infertility
Scrotal ultrasound is an examination using ultrasound that can look for testicular and epididymal abnormalities that might suggest blockage or abnormal fetal development of these structures. This is the same type of ultrasound used in pregnancy to monitor fetal development. Doppler ultrasound also checks for arterial blood flow to the testicle. Venous blood flow or varicocele presence is assessed at the same time.
Transrectal ultrasound uses the insertion of an ultrasound probe, about the size of your index finger, into the man’s rectum to look at the prostate and seminal vesicles. Enlarged or cystic seminal vesicles may be found if there is obstruction of the ejaculatory ducts.
Surgery for Male Infertility
Varicocele surgery is the ligation (tying and cutting into) of the enlarged veins to the involved testis. Some studies have shown a 70% increase in semen parameters after varicocele surgery and a 40-50% conception rate. This may not be permanent, and there is a 10-15% recurrence rate after open surgical repair and a 1-3% recurrence of the varicocele after microsurgical correction. Alternatively, this can be done intra -abdominally using the laparoscope to apply surgical titanium clips to the veins before the veins enter the inguinal canal on their way to the testicle. The interventional radiologist sometimes can block the veins by injecting small metal coils into these same veins. This technique is called embolization.
Vaso-vasostomy or epididymo-vasostomy is used to bypass blockage in the vas deferens or epididymis. There is usually a 50-75% success rate with up to a 50% fertility rate after these procedures.
Medical Treatment of the Subfertile Male
Clomid or clomiphene citrate is an estrogenic treatment first used in women to stimulate ovulation. It has been used in men with mixed results. The addition of Vitamin E 400IU per day may help the Clomid to work better than by itself. Most studies show a modest improvement in semen quality in about one third of patients treated with 25 to 50 milligrams per day for up to one year. While women cycle monthly, men can only be cycled every 3 months.
Human gonadotropin has been used as an injectable medication alone and in combination with testosterone with mixed results.
Retrograde ejaculation results in the backward flow of semen into the bladder at the time of ejaculation. Retrograde ejaculation is most common in diabetics and patients with certain spinal cord injuries or that have had surgery in the retroperitoneum. The retroperitoneum is the area in the abdomen behind all the organs. The nerves that control ejaculation are found here. Cancer surgery for testicular cancer may damage these nerves.
Medications that close the bladder neck may stop retrograde ejaculation and restore normal or antegrade ejaculation. An older antidepressant, Imipramine, at doses of 25mg twice a day may help. This has resulted in success about 38% of the time. An older antihistamine (Brompheniramine) may be used with Sudafed (Pseudoephedrine) to stimulate closure of the bladder neck and restore antegrade ejaculation. Success has been reported about 60% of the time with this combination.
Supplements suggested to assist with infertility are: Vitamin C, Vitamin E, Vitamin B12, folic acid, beta carotene, L-Carnitine, selenium, and zinc. While all have been proposed to benefit semen quality, there has not been much rigorous testing to confirm this. Some of these such as selenium have proven to be toxic in high doses.
Infertility Clinic Specialty Treatments
The following treatments are out of the normal scope of your urologist, and you will most likely be referred to the infertility clinic.
Intrauterine insemination (IUI) is the introduction of washed sperm directly into the uterus. A small catheter is inserted into the uterine cavity. This bypasses the cervical mucus and places the sperm close to the opening of the fallopian tubes. This is successful in people with low sperm counts, sperm motility problems, and retrograde ejaculation.
In Vitro Fertilization (IVF) is the fertilization of the egg outside the body in a glass (Petri) dish. After incubating the sperm and eggs for 48-72 hours, the fertilized eggs can then be inserted into the uterus, and a normal pregnancy should follow. This technique can be used in women with obstruction of the fallopian tubes due to infection, scarring, or endometriosis. It may also be used for men with low sperm counts or oligospermia. Many times, the ovaries have been stimulated to allow for the retrieval of multiple eggs at one time.
Intracytoplasmic Sperm Injection (ICSI) is the variation of in vitro fertilization that involves the injection of a single sperm directly into an egg using a microscopic needle. This technique allows even men with very poor semen quality to conceive. If azospermia is present, no sperm are in the semen, sperm may be extracted from the epididymis or testicle for use in this procedure.
Karyotyping is the medical testing of the chromosomes to look for genetic defects.
Sperm retrieval from the urine, usually associated with retrograde ejaculation, may be used as a source of sperm for these procedures.
MESA or Microsurgical Sperm Aspiration is done through a small incision with microscopic guidance of a needle into the epididymis.
PESA or Percutaneous Sperm Aspiration inserts a needle through the skin under local anesthesia to retrieve sperm. This technique does not always obtain sperm.
FNA or Fine Needle Aspiration inserts the needle directly into the testicle to obtain sperm. Frequently, there are low numbers of sperm retrieved.
Testicular Biopsy/TESA or open biopsy is occasionally utilized in the evaluation of infertility. The covering to the testicle is opened, and a small portion of the seminiferous tubules is removed. The sperm may then be isolated from this piece of tissue.
Cervical mucus testing evaluates the sperm’s ability to swim up the cervical canal into the uterus. In some instances, this mucus adversely affects the sperm, preventing progression into the uterus, often called hostile mucus.
Anti-sperm antibody testing looks for factors that kill sperm, immobilize sperm, or agglutinate sperm. Agglutination is the condition where the sperm stick together or clump together.
Hamster egg penetration testing is used to see if the viable, appearing sperm are able to fertilize an egg.
Inhibin B can be measured. If the levels are low, this may indicate blockage.
Alpha-glucosidase levels may be measured. If levels are found to be low, blockage may be present.
Chemical analysis for fructose, citrate, and zinc may be obtained.
Conclusion
Male factor infertility is a complex problem. Feel free to discuss this with your urologist. He will likely be able to counsel you about ways to improve fertility and at least begin an evaluation. If you need referral to an infertility clinic, he will be able to supply the clinic with the basic test results up to that point of your evaluation.
Male patients produce a sex hormone called testosterone. Women produce the sex hormone estrogen. It is well known that women go through menopause and quit making estrogen setting off a chain of events from hot flashes to irritability. Men go through something similar although it is much subtler in onset. Until recently, the clinical picture of andropause or Low T was poorly defined. It is now estimated that about 2.4 million men between the ages of 40-49 years have low testosterone. About 40% of men above the age or 45 years have low testosterone according to the most recent estimates.
Testosterone is produced in the testis under the influence of luteinizing hormone or LH. It then feeds back to the level of the hypothalamus to regulate gonadotropin hormone releasing hormone (GnRH), which in turn stimulates the pituitary gland to secrete LH and FSH. About 6 bursts of testosterone a day are released. Usually, there is a morning high testosterone level and an evening low testosterone level. Only 1-2% of testosterone circulates as free testosterone. The remainder is bound to albumin or sex hormone binding globulin. The normal blood levels vary widely and range from 350 to 1,198. Usually, the higher levels are in younger patients. The free testosterone is 1-3% of the total testosterone.
The symptom most men associate with Low T is erectile dysfunction or ED.
There are, however, multiple more physiologic effects of low testosterone.The whole complex is much broader in scope. Other symptoms may include the following:
Fatigue is the feeling of low energy requiring a change in lifestyle, a new onset of a sedentary lifestyle. Sedentary lifestyle may lead to an increased risk of diabetes, new or worsening hypertension, and an increase in cardiovascular conditions.
A decrease in strength or stamina either at work or in sports may occur.
Loss of muscle mass and an increase in fat are associated with Low T.
Decline in memory (cognitive dysfunction) is associated with Low T.
Onset or increase in clinical depression (mood alteration) may be a sign of Low T.
Low T leads to loss of bone mass or osteoporosis.
Loss of bone marrow stimulation leading to anemia may be found.
Low testosterone was once thought to increase the risk of coronary artery disease due to increases in cholesterol. This may have been true of oral Methyltestosterone. This drug is no longer used in the USA. More recent studies suggest that there is actually a decrease in LDL, low-density cholesterol or bad cholesterol. Triglyceride levels may also decrease. There is an increase in high-density or HDL good cholesterol.
Type 2 Diabetes and Low T appear to be linked with type 2 diabetics having double the risk of Low T over non diabetic men. About 33-50% of type 2 diabetes patients will have Low T. Type 1 diabetics do not have such an association. Type 1 diabetes patients do not lack insulin; they just develop insulin resistance. Type 2 diabetics may have a lack of insulin and testosterone production.
Obesity is associated with low levels of free testosterone. As the BMI (Body Mass Index) increases, the free testosterone decreases. Free testosterone is the most active form of circulating male hormone. This decrease in free testosterone appears to be reversible with weight loss.
Testosterone promotes muscle growth and a decrease in adipose or fat cell growth. Adipose tissue may convert some of the pre-testosterone blood factors into estrogen, which may counteract the testosterone. There may be an increase in breast enlargement and tenderness if this occurs.
Why do I have Low T?
Just as women go through menopause at different ages, there is no set age for onset of Low T. Low testosterone just happens as a part of aging. It is, however, found in men as young as their late 20s, so not all Low T is age related. Diabetics, especially insulin dependent diabetics, have an increase risk of having low testosterone. Chronic pain, requiring daily narcotics, frequently results in low testosterone. Chronic use of anabolic steroids, as used by athletes and body builders, leads to low testosterone when these high dose supplements are stopped.
Is there treatment for Low T?
Yes, there are several treatments available. While there are no pills available that are safe for long-term use, there are intramuscular injections, topical gels, subcutaneous pellets, and transdermal skin patches that work well.
The Testosterone Cypionate or ethanate shots are given into the muscle of the thigh or buttock anywhere from every 7, 10, or 14 days. Blood levels should be drawn to see if your particular dose and schedule are right for you. A peak level is drawn 48 to 72 hours after injection. A trough level is drawn the day before the next injection. These 2 levels will tell if your dose and time schedule is right for you.
The daily gels most closely mimic the normal daily cycle of testosterone production in a man. Multiple brands exist such as AndroGel, Testim, Fortesta, and Axiron. The usual doses are between 2.5gms-10gms of gel per day. All but Testim are dispensed from a metered dose pump. Testim is prepackaged in 5gram tubes. Your insurance usually dictates the doctor’s initial choice of gels. Most of these medications reach steady states in the blood stream in about 2 weeks. A blood level can be drawn to see if your daily dose is correct for you. These medications are applied to the skin of the shoulders, abdomen, thighs, or under arms. They must be applied daily to maintain a steady level.
Daily patches are available under the brand name Androderm and produce daily levels similar to the gels but may take 30 days to reach a steady blood level. The patches may be applied to any non hair-bearing place on the body.
Striant is a twice daily, buccal, mucosal patch placed in the mouth on the gums. The testosterone is then absorbed through the gums into the blood stream.
Testopel is a commercially available testosterone pellet. The pellets are placed under the skin through a small, 5mm, incision. They must be replenished every 4-6 months. This treatment requires no daily medication. Usually these are placed under the skin in the doctor’s office. The usual dose ranges from 5-10 pellets.
Benefits of Testosterone Replacement
Most men will experience a feeling of being younger or having more energy. There is a return of normal sex drive or libido. This includes better physical strength and stamina. Better memory, a sense of well being, and a decrease in depression have been observed. It does not always lead to better erections, but it can improve ED. Better quality of erection may occur.
Risks of Testosterone Replacement
As with all things in life, replacement is a calculated risk that the medicine will have a beneficial effect and not a hazardous effect.
Replacement can cause an increase in red blood cell counts causing thickening of the blood resulting in heart attack, stroke, and blood clots. This is easily monitored by a blood test, the CBC, or complete blood count.
If the man has benign prostate enlargement, testosterone replacement may cause some enlargement of the prostate resulting in a slowing of the urinary stream requiring treatment of the prostatic enlargement or BPH.
It has been proposed that long-term use of testosterone will cause prostate cancer. Other studies show that very low and very high levels of testosterone can lead to prostate cancer. Therefore, a normal level is preferred. Simple monitoring of the PSA blood tests and annual digital rectal exams will detect cancer brought to light by the testosterone replacement therapy.
Risk of transfer of the gels to women and children is usually easily avoided by the placement of the gel on skin covered by clothing. Simple contact precautions are advised. The peak absorption of most of the gels is at 4-6 hours after application. At that point, if the gel is washed off, you have still received 80-90% of your medication. Washing it off gets rid of the risk of transfer. While this is not routinely required, it may be useful in certain situations where close contact is anticipated.
There have been reports of new onset of sleep apnea with initiation of testosterone replacement therapy. Ask your partner if you snore and/or quit breathing during your sleep. If you do, this needs to be addressed prior to starting any testosterone replacement therapy.
There are some reported cases of breast enlargement and of new onset of breast tenderness in men beginning testosterone replacement therapy.
Should these conditions occur, tell your doctor. Men do occasionally develop breast cancer, and the therapy may have brought this to your attention.
Feel free to ask your urologist to explain these benefits and risks in greater detail if you have questions.
Many men are concerned about prostate health, and for good reason. If you’re a guy there is a good chance that you will eventually have some sort of problem with your prostate. The three most common prostate issues are Benign Prostatic Hyperplasia (or BPH), Prostatitis and Prostate Cancer.
Benign Prostatic Hyperplasia (BPH)
BPH is a condition that develops in men age 40 and older. BPH is a non-cancerous enlargement of the prostate gland. The older literature also describes this as prostatism and bladder outlet obstruction (BOO).
Symptoms associated with BPH usually present very slowly over time, rather than beginning acutely with sudden onset of symptoms. The related symptoms are: night time urination (nocturia), daytime frequency, slow urinary stream, hesitancy in initiating urination, intermittent or interrupted stream, double voiding and prolonged dribbling of urine at the end of urination.
Nocturia or nighttime urination is not the most bothersome symptom, but it does inhibit most people from getting to a good deep sleep pattern. Having to get up frequently in the middle of the night to urinate can cause daytime tiredness or chronic feelings of fatigue.
Overactive bladder symptoms include the sudden urge to urinate with or without the immediate loss of urine before you are able to make it to the bathroom. Also related is the frequency of urination; you have to make more trips to the bathroom because your body is voiding less urine from your bladder with each trip.
Dribbling, or continued flow of urine after urination is finished, is noted to increase as well. Even after men wait at the urinal or toilet, a wet spot may develop on their underwear, occasionally there is enough to show through to the outer clothing. Dribbling is a source of great embarrassment to many men, and it is something that you should discuss with your urologist.
Hesitancy is when you have a strong urge to urinate, but at the urinal, you have to wait to get your stream started. This is occasionally associated with straining to urinate or even sitting to urinate. Sitting may make living with some of these symptoms a little easier, but again, you should discuss these things with your doctor because the first line of treatment to reduce these symptoms is generally an alpha blocker medication.
Intermitency is the condition when the stream of urine cuts off before the end of urination but restarts a second or two later before urination is finished.
Double voiding is the pattern of urination where the stream stops in mid urination and restarts seconds later because a large volume of urine remained in the bladder. The second urination produces almost as much flow at the first urination. This is a sign of moderate or severe bladder outlet obstruction or BPH.
Diagnosis and Symptom Score Index of BPH
The diagnosis of BPH is usually a clinically based diagnosis made based on symptoms, that you have described in your history and explained to your doctor, a digital rectal exam (DRE) and a measurement of the post void residual urine, which is the amount of urine left in the bladder at the end of complete urination. (This is done painlessly in our office using painless ultrasound technology.) X-rays and blood tests are not typically needed. The DRE allows the Urologist to assess the size of the prostate as well as the symmetry, and consistency of the gland.
We put the BPH Symptom Score Index here for you to print out and bring to our office. Obviously, we are here to help you and our new patients print these out and bring them in on a regular basis. However, if you are not close enough to visit us the Symptom Score Index will help any urologist with their assessment of your symptoms.
Treatment of BPH
Alpha-blockers were originally used as high blood pressure medications in the 1980’s, but studies conclusively showed that they helped the prostate gland as well. Because alpha-blockers helped the prostate gland, they were refined to try and eliminate the lower blood pressure that the original alpha-blockers caused while preserving the benefits to the prostate. Alpha-blockers essentially work by relaxing the muscular fibers in the prostate itself. Examples of commonly used medications are Flomax (Tamsulosin), Uroxatral (Alfuzosin), Cardura (Doxazosin), Hytrin (Terazosin), and more recently Rapaflo. All are once daily medications. Most patients will see a difference in urination within 5-14 days. Side effects include stuffy nose, low blood pressure on rapid standing (also called orthostatic hypotension), rarely fainting, and retrograde ejaculation (“dry ejaculation” since the semen goes backwards into the bladder instead of out the penis).
The second line medications work by physically shrinking the prostate. These medications work to accomplish prostate size reduction by blocking the conversion of testosterone into dihydrotestosterone. Dihydrotestosterone is the active hormone stimulating prostatic growth. These medications leave testosterone intact thus avoiding sexual dysfunction in most people. This group of medications includes Proscar (Finasteride) and Avodart (Dutasteride). They must be taken continuously because they take months to work. (Proscar takes 6-12 months for maximal effect on the prostate size. Avodart takes only 3-6 months to work.)
There are two main pathways for the conversion of testosterone into dihydrotestosterone. About 80% of men utilize the main pathway that is blocked by the Proscar. Avodart blocks both the primary and secondary pathways. This more complete blockade accounts for its quicker onset of action.
Combinations of Flomax and Dutasteride are also available; the brand is Jalyn. The benefits of relaxation begin in a few days and help until the 3-month affect of the Dutasteride takes effect.
A Note About Supplements for Prostate Health
The original idea for the prescription medications is based on the observation that SAW Palmetto berry extract and Africanum Pygeum relieved symptoms of outlet obstruction. The European data shows these to be effective medications. However, it should be noted that the European equivalent of our FDA monitors manufacturing quality by makers of supplements while the supplement industry is nearly totally unregulated in the USA. Several independent assays of the ingredients have shown that the label does not always reflect what is in the bottle. Therefore, it is difficult to recommend any over the counter (OTC) supplement due to lack of quality control in the USA.
The way I see it, if the Mars Candy Company didn’t put 12oz of M&Ms in a 12oz bag, it should be considered fraud. If Coke didn’t put 12oz of Coke in a 12oz can, it should be considered fraud. The FDA regulates these guys, and guess what, you get what is on the label (with very little +/- but acceptable variance). Look at the recent Subway scandal. Your “foot-long” sandwich was really only 11.5 inches long. While that doesn’t sound like much, across the number of franchises, they saved a lot of money by short-changing their customers. With supplements, no one is looking. One only needs to look at the recent string of scandals in the Chinese manufacturing industry (lead found in children’s toys and jewelry, melamine chemical in plastic found in milk and milk products) to see my concerns. It has been demonstrated over and over and over via scientific testing using rigid standards of consistency that quality in OTC supplements is questionable from one manufacturer to the next, from one bottle to the next, and from one pill to the next. I suspect that if no one was looking the premium gas at the pump may actually be regular gas at an inflated price. Do you really want to take that kind of chance with your health if you have a specific medical condition that requires a very specific dose of medication to keep it under control?
Look, I have nothing personal against the use of supplements, and as a physician, I certainly need to know if you take any before deciding on a course of treatment for you. I just worry about anyone spending money (and in some cases it’s a lot of money) on these supplements. Your money may be wasted on inadequate doses, low quality ingredients, or you may simply be getting “snake oil”. (This sort of thing has been around for hundreds of years, yet it is still a modern problem because there will always be a demand for it.)
Minimally Invasive Procedures for Benign Prostatic Hyperplasia
A quick note here – any time you hear your surgeon use the term minimally invasive – listen up. Procedures and techniques have changed drastically over the past 30 years. More and more minimally invasive procedures are done now than ever before because of the quicker recovery time to the patient and the reduction of risks or complications to the patient from the procedure.
Minimally invasive surgical procedures have been employed to treat BPH in an attempt to achieve more symptomatic relief without the side effects of transurethral resection of the prostate or TURP (often referred to as a “roto-rooter” procedure). TURP is the procedure your dad and his dad were afraid of.
The two most common office based minimally invasive procedures are transurethral microwave thermotherapy (TUMT), which is the heating of the prostate with microwaves, and transurethral needle ablation (TUNA).
Both of these minimally invasive procedures use heat generated by microwaves and radio waves respectively to shrink the central portion of the prostate thus allowing the flow of urine from the bladder to the toilet once again.
Three Surgical Options for BPH are:
1. Visual Laser Ablation of the Prostate (VLAP)
VLAP is an appropriate procedure for most men with glands below 60-70cc. The size of the prostate does place some limitations on the procedure. Most normal prostate gland are small and measure about 15 cubic centimeters (cc). The range of BPH enlargement is between 30and 500cc. Luckily, most obstructing prostates are below 100cc of enlargement. It is possible on the larger 100cc glands to do these in 2 stages. This does require two different operative sessions and therefore increases the cost.
Watch Patients discuss BPH and Treament with GreenLight laser.*
Both of these learning materials are from the AMS GreenLight website.
While most men put off prostate surgery until there are absolutely no more medical options, almost all are happy several months after the surgery and tell me how they wished they had done this sooner. Most have the stream of a much younger man and because of decreased nocturia, sleep better. This uninterrupted sleep leads to less fatigue and more energy. Most no longer have to go to every restroom they pass.
Laser ablation of the prostate, Greenlight laser or Evolve laser, is a well tolerated procedure that is usually out-patient. Most patients have a catheter for only one day. Most patients are able to drive themselves to the doctor’s office the next day. There is a recovery of 2-6 weeks depending on the degree of lifting and straining you do at work with most people being back to work in 2 weeks. This procedure does not produce any tissue samples for evaluation for cancer. If the PSA (prostatic specific antigen) is normal, no tissue is required. If the PSA is abnormal, a preoperative prostate biopsy may be obtained by your surgeon. The laser generates a very intense beam of light emitted from the end of a side-firing laser fiber. The light usually comes out the side at a 70 degree angle; this is slightly forward and protects the external urinary sphincter in the later part of the operation. The laser essentially boils the water from the tissue vaporizing the tissue. It generally seals the vessels as the resection continues thus minimizing bleeding. Usually, this results in 2-3 ounces of blood loss. Because the laser allows for the use of saline, the post TUR syndrome is avoided. Rarely is a transfusion needed, and the risk of anemia and fatigue from anemia is very small. Since there is little bleeding, the operation is usually out-patient. Most of the time, a catheter can be removed in 24 hours. I have my patients remove their catheter the following morning after surgery and to come see me in the office the next afternoon to assure proper voiding and to rule out retention of urine. One in 10 might need reinsertion of their catheter for 1-2 more days. One can care for daily living activities without fear of complications. Restrictions on lifting are for 2-6 weeks and are affected by the usage of blood thinners.
Most men worry about erectile dysfunction (ED or impotence) when considering prostate surgery for prostate enlargement or benign prostatic hyperplasia (BPH). It should be noted that this is most common with prostate cancer surgeries, and there is minimal risk with surgery for BPH. The minimally invasive procedures that generate heat such as Green Light laser or Evolve laser, TUNA (transurethral needle ablation), and transurethral microwave thermotherapy (TUMT) have a very low occurrence of ED in the 1-5% range depending on the type of surgery.
ED with surgery for BPH occurs almost exclusively in men already experiencing moderate to severe ED preoperatively. The incidence of ED is higher with a TURP possibly due to the electricity used for cutting the prostate tissue. The electricity courses out through the periprostatic nerves to a grounding pad. Open or incisional prostatectomy for BPH is also more likely to cause ED than are transurethral surgical procedures. Open surgeries are more likely to damage the nerves on the outer surface of the prostatic capsule and result in ED.
Another common concern among men undergoing prostate surgery for BPH is stress urinary incontinence or SUI. This type of incontinence occurs in only a small percentage of TURP procedures and is less common in the minimally and less invasive procedures. This is most common in men with long-standing urinary obstruction and urinary retention. This usually resolves with a few months of time. This type of problem is due to the external urinary sphincter getting lazy due to the prostatic blockage. If the prostate is blocked, then this muscle doesn’t have to work and temporarily loses some of its strength; this muscle must be exercised to stop the SUI. Kegel’s exercises help return the external urinary sphincter to its normal function and stop the stress incontinence. Kegel’s exercises are often used in women after childbirth to regain bladder control and stop postpartum SUI.
Complications of laser procedures are transient dysuria or burning with urination (6%), delayed hematuria or blood in the urine (3%), bladder neck contracture or blockage due to scar tissue (2%), and retention of urine or inability to urinate the first time the catheter is removed (1%). No incontinence or newly developed impotence was reported in most studies, and in the studies reporting ED, it is 1-3%. However, up to 26% of the sexually active men experienced retrograde ejaculation also called dry ejaculation or no ejaculation of semen postoperatively. While this does not cause any physical problem, it is psychologically stressful to some men. Retrograde ejaculation is a side effect of all prostatic surgeries and alpha-blocker medications such as Flomax/Tamsulosin.
Over the past 10 years, I have almost completely replaced transurethral resection of the prostate (TURP) in my practice with Green Light laser visual laser ablation of the prostate (VLAP). Almost everyone who is suitable for TURP is suitable for laser vaporization also called photo vaporization of the prostate (PVP).
I am just now starting to re-operate on some of the first laser patients that I did 10 years ago. The oldest patients that I have done are 89 and 93 years old. They were in urinary retention and wearing a catheter. They are both still very active.
As compared to TURP:
The procedure is practical in most men with a prostatic gland size up to 80-100cc or about 3 ounces of tissue.
There is significantly less blood loss with laser prostatectomies. As of 2016, none of my patients have required blood transfusion or readmission to the hospital.
The average blood loss from a TURP is 500ml or 1 pint of blood. The transfusion rate for TURP is about 5-7% currently, but in the past, it has been much higher.
There is no hospital stay with laser surgery of the prostate, and there almost always is a hospital stay with TURP.
There is a rapid improvement in urine flow noted by the American Urological Association (AUA) symptom scoring after laser surgery.
There is a shorter period of catheterization with Green Light laser PVP. The catheter is usually removed in 24 hours or less.
There is a much quicker return to normal activity with Green Light laser versus TURP. Most men can resume most normal activity by 2 weeks. After Green Light laser, most men can drive the following day and are advised not to lift or strain for 2 weeks, or there is an increased risk of delayed bleeding. TURP patients are advised not to lift for 4-6 weeks.
There is as little as 1% risk of developing ED in the later studies versus an initial reported rate of 3-5%.
The laser surgery has a shorter anesthetic time, and on average, the procedure from start to finish is 60-90 minutes in the operating room.
The Green Light laser procedure is usually shorter and therefore costs less than a TURP in most cases.
Because the fluid absorption is so much less than with a TURP, there is little or no risk of post-TUR syndrome. TUR syndrome consists of fluid overload from absorption during the TURP, congestive heart failure, and dilutional hyponatremia with confusion. Since the risk of intraoperative fluid overload is so low, older men that would be assigned to have a chronic indwelling Foley catheter with monthly catheter changes are now able to have prostate surgery.
As of 2011, there had been >200,000 Green Light laser surgeries performed worldwide.
The GOLIATH study (2014) done at 29 hospitals in 11 European countries directly compared the results of Green Light to TURP in 269 men and confirmed the safety and equivalency of laser treatment. The improvement in AUA symptom score and PSA decline in both TURP and Green Light laser were equivalent.
In conclusion, while medication is the initial main treatment for most men with BPH, once those medications no longer work, men have a safe and effective surgical procedure that is durable and as good as TURP with fewer complications and risks of ED or incontinence as compared to TURP.
2. Transurethral Resection of the Prostate (TURP)
TURP has the next longest recovery, but there is no skin incision. The TURP procedure relies on an electric cutting loop to cut out or resect the tissue. The chips, as these tissue fragments are called, are pushed into the bladder and are later retrieved for pathologic tissue evaluation. Complications include bleeding with resultant anemia and frequently require blood transfusion. The procedure usually requires several days of hospitalization and catheterization. The recovery is 6-8 weeks. The most serious intraoperative complication is the TUR syndrome. This complication results from the replacement of blood lost with a non-sodium containing fluid. This can lead to electrolyte imbalance with decreased serum sodium and potassium. This syndrome leads to swelling in the brain and confusion intra-operatively. The surgeon must stay aware of blood volume lost, the fluid used, and he must communicate well with anesthesia during the procedure. It results in a pint of blood loss in most people not requiring transfusion but does cause some temporary fatigue and weakness. The time to return to work is usually 4-6 weeks with very limited homebound activity for 1-2 weeks. Catheters are usually used 2-5 days. Required hospitalization is 1-3 days.
3. Open Prostatectomy
The best procedure for long-term symptom relief is the open removal of the central portion of the prostate. While this is the gold standard for symptom relief, it is also the most invasive, and it carries with it the longest recovery time. The open prostatectomy is now reserved for only the largest prostate glands.
This requires an incision made in the lower abdomen to access the prostate. Once the surface of the prostate is cleaned, the capsule is opened, the urethra divided, and the prostatic adenoma is enucleated. The bleeding may be quit brisk resulting in the loss of several units of blood. The capsule is closed, and a urethral Foley catheter is placed; sometimes, a suprapubic catheter is utilized as well. The normal hospitalization stay is 4-7 days with no work for 6 weeks. Bloody urine is quite common for several weeks. Blood clots causing obstruction and the inability to urinate in the first 2 weeks postoperatively are moderately common leading to ER visits for repeat catheter placements.
Prostatitis (Inflammation of the Prostate)
Prostatitis is the male equivalent of the female UTI or cystitis. Prostatitis is, however, much less common than a UTI is in women. The symptoms of both are similar and consist of new onset of frequent urination, sudden urge to urinate, an increase in nighttime urination, and possibly blood in the urine. In addition to the symptoms UTIs and prostatitis have in common, there are some that are only present with prostatitis. These consist of blood in the semen, painful ejaculation or dyspareunia (painful intercourse), new or sudden onset of erectile dysfunction (ED), or an increase in severity of mild ongoing ED. Occasionally, there will be acute urinary retention (the inability to urinate). Slowing of the stream while on medications such as Tamsulosin may occur.
If the symptoms are ignored and the person continues to work at a strenuous job, the infection may reflux down the vas deferens and cause epididymitis. This is very painful as it results in acute swelling of the scrotum on the affected side. It becomes difficult to walk due the pain that it causes each time the testicle brushes against the thigh.
The cause of prostatitis is debatable. Many people are told it is due to a lack of frequent enough sexual activity while others are told they are too sedentary. Another group of patients that I see prostatitis in are men that work in construction. This patient group has a physically demanding job with no set starting and stopping times with an irregular break and lunch schedule.
The two stereotypical examples of people that hold their urine are truck drivers (or really anyone that has to sit for very long periods of time without getting up) and manual laborers. Many truck drivers put off urination until they have reached their destination or scheduled stop. The laborer with a full bladder keeps lifting and straining, all the while putting off urination, until either the job is done or until the next break. This requires that he hold back the urge to urinate for extended periods. Each time he stops a significant urge to go, they are pressurizing the prostatic urethra. In doing so, they set the stage for prostatic inflammation. This inflammation may turn into infection from time to time. I believe the two different people have one thing in common and that is holding their urine and delaying urination.
There are two urinary sphincter muscles that act as control mechanisms between the bladder and the outside of the body. The first one is close to the bladder and in the bladder neck. It is the internal sphincter. The internal sphincter is what keeps babies dry between diaper changes. (Without it, babies would constantly drip urine as it was produced and put in the bladder.) The external sphincter is the toilet training muscle, and it is positioned below the prostate. When you stifle urination and force the urge to urinate to go away, you are pressurizing the prostatic urethra. Sometimes, by doing this, the very acidic urine can cause inflammation of the prostate, and this can set the stage for a possible prostatitis.
Treatment consists of antibiotics, scrotal support, ice (initially), and heat (later). The time course is much different in men’s prostatitis than in women’s UTIs. Women may be treated with 3-5 or even 7 days of antibiotics depending on age, associated illness, and frequency of their UTIs. Men are treated for 2-4 weeks or even as long as 6-12 weeks. The difference is that women are treating a urine infection that empties with each trip to the toilet. The germs are diluted as they are killed by the antibiotics. The antibiotics in women are excreted in the urine as a waste product and may reach 200 times the achievable concentrations of antibiotics in the blood stream. Men, however, are treating a tissue infection and must rely on blood levels of antibiotics alone. At these lower levels of antibiotic concentrations, mean inhibitory concentrations or MIC for short, takes much longer to clear the bacteria from the tissue than it does from urine. The larger the prostate the longer it takes to clear the infection. Associated conditions such as increased post-void residual urine or incomplete empting prolong the treatment as well.
Antibiotics are merely chemicals that kill bacteria but do not harm the person taking them. Most bacteria have a favorite acid or basic environment to work in, or favorite pH. Most infected tissues are acidic or have a low pH; prostatic tissue may have a more basic pH when infected. At a pH of 7-8, the same antibiotic does not work as well as it might at an acid pH of 5-6. This also prolongs the treatment of prostatitis. The lipid membranes in the prostate may also prevent the large molecules of common antibiotics like Sulfa drugs, Bactrim, and Septra from crossing readily into the cells.
The oldest treatment (before around 1960) prior to the invention of antibiotics for prostatitis was the digital rectal prostate massage (DRE). Men would go to the doctor sometimes 2-3 times a week for a rectal massage of the prostate. The fluid expressed from the prostate would give temporary relief from the symptoms of prostatitis. This may be where the notion that regular ejaculation prevented prostatitis comes from. It surely plays into the psyche of men “needing” regular intercourse to prevent problems and infections of the prostate. A study in 2006 concluded that prostate massage did not improve outcomes for treatment of prostatitis and that antibiotics alone should be used to treat prostatitis.
The most common antibiotics used today for the treatment of prostatitis are the Quinolone antibiotics such as Cipro (Ciprofloxacin), Levaquin (Levofloxacin), Sulfamethoxazole / Trimethoprim (Bactrim, Septra), Vibramycin (Doxycycline), and occasionally Cephalosporins such as Keflex (Cephalexin)
The urologist will evaluate you for conditions predisposing you to infections. Risk factors include incomplete emptying due to urethral strictures, scarring in the tube through the penis, prostate enlargement or BPH, bladder stones, diabetes mellitus, and medications such as immunosuppressants, the most common of which are steroids and other chemotherapeutic agents. The occasional prostatitis that clears rapidly needs only an office evaluation. The recurring types need more in-depth evaluation and may require cystoscopic evaluation of the urethra, prostate, and bladder. Radiographs such as CT scanning may sometimes be a part of the evaluation.
Prostate Cancer
According to the Centers for Disease Control and Prevention (CDC), the top diagnosed cancer among men in the United States is prostate cancer. In 2007, there were 223,307 men diagnosed with prostate cancer, and 29,093 men died from the disease. Prostate cancer is also the second leading cause of cancer deaths in men after lung cancer. (The top three cancers in men are lung, colon, and prostate.) Early diagnosis of cancer is the basis of all other advances in the treatment of breast cancer, cervical cancer, colon cancer, and lung cancer, and studies have shown that the earlier the these cancers are diagnosed in a patient the better the survival rate is for that patient. The CDC study I referenced earlier also added, “Since there is not enough medical evidence to decide if the potential benefits of prostate cancer screening outweigh the potential risks, the CDC supports informed decision making.”
Having seen men’s reluctance to have a digital rectal exam and the dismal history of DREs at early detection of prostate cancer, the prostatic specific antigen or PSA was invented. This has been used in conjunction with DREs over the last 20 years to find prostate cancer in its earlier form.
Left-side: Advance Carcinoma of the Prostate C, Right-side: Healthy Prostate and Bladder
Left-side: Healthy Prostate, Right-side: Early Carcinoma of the Prostate
There are several prostatic conditions that may elevate PSA. These include benign prostatic hyperplasia or BPH, prostatitis, and prostate cancer. Larger prostates have more PSA than smaller ones. The amount of PSA per cubic centimeter or cc of prostatic tissue is called the PSA density. The PSA velocity is the amount of rise over a period of time; all of the conditions above are used to evaluate men for signs of prostate cancer. There are no early warning signs of prostate cancer. A prostate biopsy is used to obtain tissue from the gland to look for prostate cancer cells. Prostate cancer can not reliably be found on rectal exam, CT scans, or MRI.
Recently, the US Preventive Services Task Force has recommended that doctors stop using PSA as a screening tool for prostate cancer. They found no benefit in survival of men found in the early stages of prostate cancer by PSA. They alleged that screening does more harm than good. This seems contrary to what occurs in the treatment of all other cancers found in the early stages. Many primary care physicians stopped doing digital rectal exams in favor of PSA. Now that there is a recommendation to stop doing PSAs, they have not resumed DREs, thus abandoning all efforts to find prostate cancer. If your doctor is not at least discussing PSA and doing a DRE, you to ask your physician for an exam.
Breast cancer is the analogous cancer in women to prostate cancer in men. Both are mediated by hormones, estrogen in women and testosterone in men. Women receive a breast exam and a mammogram, while men need a DRE and a PSA. Family history of either of these cancers increases the risk for other family members. Some studies have suggested that the same chromosomal mutations may be responsible for both cancers. The earliest medical treatment attempts in both were manipulations of these hormones. If either a woman with a breast mass or an abnormal mammogram or a man with an abnormal DRE or PSA is found, both require biopsy for diagnosis. CT scans and MRIs are used for staging after biopsy but are not reliable enough for diagnosis. Of course, not all biopsies will be positive for cancer. In men, about 25% of people with a PSA between 4-10ng/ml will have a positive biopsy. There is a similar positive rate in breast biopsy. Now critics of PSA say that if only one is positive that the other 3 were “unnecessary”. How can they be unnecessary if there is no other test to find the cancer? In women all biopsies appear to be necessary even though many find benign breast conditions. Many women have had 2, 3, or even 4 breast biopsies in their lifetime.
Conventional wisdom says that all men have a small amount of prostate cancer, so what’s the big deal since you always “die with prostate cancer and not of prostate cancer”? In the 1960’s, the life expectancy of a male was about 65 years. So if a man with medical problems was diagnosed with cancer at age 55-60 years, it is true that he may very well die of other causes. Now that the life expectancy is 76.5 years with an upward range of 90 years, it is not true of relatively health people diagnosed at an early age (less than 70 years old). In people with a 10-15-year survival, there is a 44% reduction in deaths in the screened early stage prostate cancer group.
There are about 30,000 prostate cancer deaths each year in the USA, and there are 240,000 newly diagnosed cases of prostate cancer per year. Men over 50 years of age, the age group most at risk, make up about 25% of the male population, about 10 million men, in the USA. One man in 36 will die of his cancer. While the USPSTF found no benefit to prostate cancer screening in the USA, the ERSPS or European Randomized Study for the Screening of Prostate Cancer found a 21% decrease in the risk of death from prostate cancer in the PSA screened group. The Göteborg trial found a 40% reduction in prostate cancer death in the age group of 50-64 year olds with a 14-year survival. There has been noted to be a 44% reduction in prostate cancer related deaths in the USA over the last 20 years. The SEER data shows a 75% reduction in the presentation of men with advanced stage disease. The survival in localized prostate cancer is about 72% while the survival for metastatic disease at 10 years is only 3%. Screening has lowered the number of men presenting with advanced stage or metastatic disease by 75% over the last 20 years. Metastasis is the advanced state of a cancer where it has spread distantly from the primary site. In prostate cancer, this spread is typically to bone.
Some groups are at greater risk of prostate cancer. These include African Americans and anyone with a family history of prostate cancer. Even if random screening is found to be of no benefit to men in general, which I find unlikely given the increase in average life expectancy, targeted screening of these groups should continue.
All cancers are not aggressive. Your doctor tries to take this into account if your biopsy is positive. An informed decision to treat or watch a cancer is a complex decision best discussed with your urologist. I personally do not recommend treatment for small prostate cancers in all patients. Some patients benefit from a “wait and see” approach or watchful waiting. Watchful waiting is also called medical monitoring in some articles. This involves serial monitoring of PSA and DRE to try to pick out the cancers with the aggressive growth patterns for treatment and the slow growing ones for close monitoring. If an initially slow growing cancer changes to a more aggressive growth pattern, some people then decide to change to a treatment and quit the monitoring group.
Your urologist should help you understand that he takes into account the grade of the tumor or Gleason score, the TMN stage of the tumor, the PSA, the volume of tumor, stated as the number of cores positive for cancer from your biopsy, and whether it is unilateral or bilateral. He should consider your family history of longevity, and he should speak to your family doctor about your overall health and consider whether you will live another 10 years or more. People with multiple medical illnesses not expected to live another 10 years should seriously consider monitoring over treatment of a small, non-aggressive, prostate cancer.
The goal of treating prostate cancer is not just to cure it but to decrease the morbidity and to evaluate the decrease in the overall quality of life associated with incurable prostate cancer. The spread to bone is often quite painful. The chemical castration treatments cause significant decreases in quality of life evaluations. These treatments can routinely cause hot flashes, night sweats, muscle weakness, osteoporosis, and cognitive decline. While urologists realize that there is certainly a downside to treating prostate cancers with surgery and radiation, doing nothing is not often a good option either.
The recent discussion seems to favor going back to the pre 1980’s non PSA era when 16.9% (T1) was the percentage of early stage prostate cancer; 48% were T2. T1 is now about 50% (early stage cancer now) and 27% T2. Certainly there has to be some happy median between the treatment for all and no treatment for anyone.
Prostate Cancer Grading
Prostate cancer is graded using the Gleason score. This score factors in a two-part grade, a nuclear grade, and a glandular grade. The glandular grade has to do with the architecture of how the glands are put together on the biopsy specimen while the nuclear grade looks at the nucleus of the individual cells for clues of how aggressive that cancer may be. An example would be a 3+4/10 or grade 7/10. The system allows for more categories to tell how aggressive the tumors usually act. A grade 3+4 is a less aggressive tumor than 4+3, although both are grade 7. The later 4+3 acts more like a grade 8/10 cancer.
Staging of Prostate Cancer
Localized Prostate Cancer
This implies that the prostate cancer is confined to the prostate gland and has not spread outside the prostatic capsule, no spread to the regional lymph nodes, or distant metastasis to bone.
Local Spread of Prostate Cancer
This is spread detected in the surgical pathology specimen and has typically spread just beyond the prostatic capsule but not into the regional lymph nodes.
Distant Spread of Prostate Cancer
This indicates spread to the lymph nodes out of the pelvis and/or into the bone.
Staging the cancer after needle biopsy utilizes a bone scan when the PSA is grater than 20.0 and the Gleason score is 8 or greater. The bone scan is a radio nucleotide scan that marks areas of bone that are abnormal and need further evaluation by standard x-rays or MRI. This typically exposes the person to less ionizing radiation than they would get using multiple plain x-rays.
Computed Tomography Scanning (CT scan, which is sometimes called a CAT scan) is used to evaluate the pelvic area for signs of pathologically enlarged lymph nodes. These are typically lymph nodes greater than 10 millimeters in diameter.
Magnetized Resonance Imaging (MRI) is currently used in staging prostate cancer, evaluating suspicious boney lesions, or for guiding prostate biopsies but not currently for diagnosing prostate cancer.
Prostate Cancer Treatment
Watchful Waiting of prostate cancer:
This act of diagnosing prostate cancer but not treating the cancer is called watchful waiting. Through mutual agreement between the patient and the urologist the patient undergoes regular DRE and PSA testing. This is most often reserved for older, sicker patients with small amounts of cancer on biopsy. They typically have lower Gleason score cancers. If the cancer shows signs of progression, then treatment may be initiated at the time of progression.
Medical Monitoring of prostate cancer:
Medical monitoring is very similar to watchful waiting, but in addition to monitoring PSA and DRE, it usually adds a follow-up prostate biopsy. If the second biopsy shows an increase in tumor volume or increase in Gleason score treatment is again discussed
External beam therapy:
External beam therapy is the use of radiation generated by a linear accelerator to produce the wavelength of radiation needed to treat the prostate cancer. This is usually given in daily fractions Monday thru Fridays for 8-8.5 weeks. It may be aided by the insertion of gold fiduciary marker seeds to guide the radiation therapy. The prostate rises when the rectum is full of stool or gas, and the bladder may change position based on its degree of fullness. The marker seeds allow the therapist to change the depth of treatment from day to day to accommodate these changes in position. This is used to avoid damage to the bladder and rectum.
Seeds/Brachytherapy:
This is the treatment of prostate cancer by insertion of radio active seeds or pellets directly into the prostate. Both Iodine 125 and Palladium 103 are used. This delivers a higher dose of radiation to the prostate than can be delivered by external beam (EBRT) with no increase in side effects.
Radiation plus Hormonal Deprivation:
Tumors with higher grades and PSAs have a greater tendency to recur. In an attempt to stop the recurrence, LH-RH (Luteinizing Hormone-Releasing Hormone) inhibitors were given to the patient before the radiation therapy. LH-RH inhibiting factors affect the pituitary to stop the release of LH. LH is the hormone that stimulates the testicle to produce the testosterone. By blocking this hormone, testosterone levels fall to 30ng/ml, which is the same as castrate testosterone levels. Starting with the LH-RH medications before onset of ERBT weakens the cancer cells and makes them more sensitive to radiation induced cell death. Initially, 3 years of LH-RH were used. Then 2 years of LH-RH plus antiandrogens were shown to be as good. Now some patients require only 3-4 months of LH-RH and antiandrogens reserving the longer course for patients with grade 8 or with a PSA greater than 20.0.
Combined EBRT and Brachytherapy:
For higher grade tumors with higher Gleason scores, higher PSAs, and more volume of tumor, the EBRT may be used to treat the area outside the prostatic capsule while using brachytherapy seeding to increase the dose to the center of the prostate gland.
Radical Prostatectomy:
This is the removal of the prostate by surgical means. The prostate is disconnected from the bladder, the prostatic urethra, and the rectum. A nerve sparing technique is to preserve the nerves responsible for erection. This avoids causing ED
Retropubic Prostatectomy:
This approaches the prostate through a small 4-5 inch incision beginning over the pubic bone at the base of the penis and extends upward. This is the approach preferred by about 90% of surgeons. Nodes can be sampled in this technique.
Perineal Prostatectomy:
This approaches the prostate through a transverse incision behind the scrotum but in front of the anus. The nerve sparing technique is also employed. Nodes cannot be sampled using this approach.
Robotic Retropubic Laparoscopic Prostatectomy:
Robotic retropubic prostatectomy utilizes a surgical robot to assist the surgeon. The advantages are that the laparoscopic approach uses a smaller incision and there is significantly less blood loss. The anastomosis or closure of the urethra to the bladder can be seen more easily. There are conflicting reports as to whether this procedure actually causes less incontinence and erectile dysfunction than does the open procedure. The learning curve for the robotic surgeon is stated to be about 100-200 cases before the rate of leaving a positive margin decreases to that of an open surgery. Many university trained surgeons now come out of training with this number of cases. The implication of a positive margin is that cancer has been left behind, and the patient may need additional therapy such as follow-up postoperative EBRT.
Incontinence
Stress versus Urge Incontinence:
Incontinence is defined as leakage of urine. There is stress incontinence such that when one coughs, sneezes, or moves suddenly urine comes out unexpectedly. This is most common after surgery and usually goes away as healing continues over 4-12 months. Treatment options include Kegel exercises to strengthen the external sphincter, biofeedback, and surgical sling procedures.
Alternately, there is urge incontinence with loss of urine accompanied by the sudden urge to urinate and the inability to stop the initiation of urine flow. Multiple medications are available for treating this problem. The most common side effects of these anticholinergic medications are dry mouth and constipation. This type of incontinence is most common after radiation therapy and most often goes away over 4-12 months.
Erectile Dysfunction (ED)
Delayed versus Immediate:
Immediate ED is found in up to 80% of prostatectomy patients. The ED improves over the first postoperative year with about 50-80% recovery in the ability to resume intercourse. The resumption of intercourse may require the use of medications such as Viagra(sildinafil), Levitra(vardenafil), or Cialis(tadalafil) Attempts to speed the return of normal erections include starting these medications in the immediate postoperative period. They usually begin as soon as 2 weeks postoperatively. Intracorporeal injection of vasoactive medications has been tried as well. Medications such as prostaglandin E1 (brand name Caverject) and Edex are used. Older mixtures of Phentolamine and Papaverine, or occasionally Trimix (a mixture of prostaglandin E1, Phentolamine and Papaverine) are the most commonly used medications. Some studies have recommended the use of vacuum erection devices for the return of erectile function.
Positive Margins on a Pathology Specimen
If the pathology specimen has a positive margin, meaning some of the cancer may have been left behind, then close follow-up with serial PSA tests are used. The first PSA is taken 6-8 weeks after the surgery. If the PSA fails to fall below the level of < 0.015ng/ml, then cancer cells are present and are producing PSA. At this point, additional treatment may be offered in the form of External Beam Radiation Therapy (EBRT). For the best results, the EBRT should be administered before the PSA reaches a level of 1.0ng/ml. Surgical removal of the prostate devitalizes a small rim of tissue around the prostate. This area dies back for several millimeters. If the margin containing the cancer was small, this zone of tissue death may kill the rest of the cancer. About 30% of positive margin patients normalize their PSA to less than 0.015ng/ml. They usually do not require EBRT treatment.
Biochemical Recurrence/ Metastasis:
A rising PSA, after it initially returned to nearly zero, is indicative of the cancer coming back. In the presence of a positive margin, a negative bone scan, and negative CT scan, it is assumed that it is a recurrence in the pelvis and probably will respond to EBRT. This rise in PSA can occur as long as 11 years after having a negative margin pathology specimen and undetectable PSA. While most recurrences are found in the first 5 years, long-term monitoring is required.
Hormonal Therapy:
Prostate cancer, much like breast cancer, is most often sensitive to hormonal deprivation therapy. The male hormone is called testosterone. Lowering of testosterone was first found to treat metastasis to bone with bone pain in the 1950s. Hormonal deprivation, in the 1950s, was accomplished by removal of the testicles otherwise known as castration. In the 1980s, Luteinizing hormone-releasing hormone inhibitors, LHRH for short, were used to block the pituitary hormone LH. The testes no longer had to be removed to treat the cancer. The medication simply turned off the production of testosterone. Several drugs are available including Lupron, Trelstar, Eligard, and Zoladex. While at first requiring monthly injections, the drugs now come as 3, 4, and 6 month preparations.
Side effects include menopause-like symptoms of hot flashes, night sweats, agitation or depression, and osteoporosis may occur.
Antiandrogens:
Some testosterone is made by the adrenal glands, and this accounts for a small portion of the total testosterone. If normal testosterone is 350 to 1,198, the castration levels are about 30ng/dl. This small amount of testosterone from the adrenal glands, may be enough to keep the cancer growing. Antiandrogens attach to the testosterone receptors and block the body’s use of the remaining available low testosterone.
Chemotherapy for Hormonal Resistance
Currently, several chemotherapies are available for patients failing standard hormonal therapy. These patients are said to have castration resistant prostate cancer and it is hormonally insensitive. Discussion of these types is beyond the scope of this article.
Taxotere (Docetaxe) l and Zytiga (Abiraterone) are the two chemotherapies given by oncologists but these are both beyond the scope of this article.




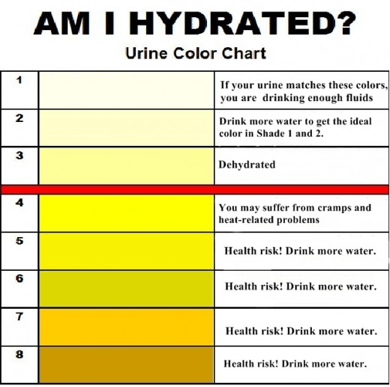



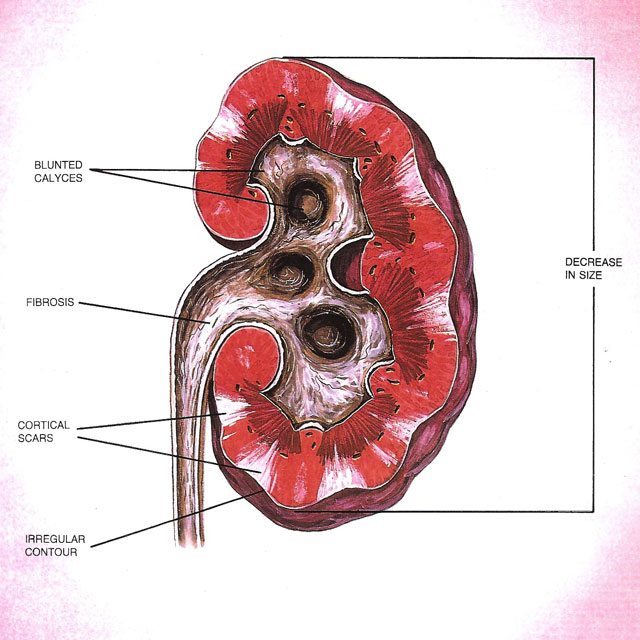
 Male patients produce a sex hormone called testosterone. Women produce the sex hormone estrogen. It is well known that women go through menopause and quit making estrogen setting off a chain of events from hot flashes to irritability. Men go through something similar although it is much subtler in onset. Until recently, the clinical picture of andropause or Low T was poorly defined. It is now estimated that about 2.4 million men between the ages of 40-49 years have low testosterone. About 40% of men above the age or 45 years have low testosterone according to the most recent estimates.
Male patients produce a sex hormone called testosterone. Women produce the sex hormone estrogen. It is well known that women go through menopause and quit making estrogen setting off a chain of events from hot flashes to irritability. Men go through something similar although it is much subtler in onset. Until recently, the clinical picture of andropause or Low T was poorly defined. It is now estimated that about 2.4 million men between the ages of 40-49 years have low testosterone. About 40% of men above the age or 45 years have low testosterone according to the most recent estimates. Many men are concerned about prostate health, and for good reason. If you’re a guy there is a good chance that you will eventually have some sort of problem with your prostate. The three most common prostate issues are Benign Prostatic Hyperplasia (or BPH), Prostatitis and Prostate Cancer.
Many men are concerned about prostate health, and for good reason. If you’re a guy there is a good chance that you will eventually have some sort of problem with your prostate. The three most common prostate issues are Benign Prostatic Hyperplasia (or BPH), Prostatitis and Prostate Cancer.